

GM Muraca,a,b,c A Skoll,b,c S Lisonkova,a,b,c Y Sabr,b,d R Brant,c,e GW Cundiff,b,c KS Josepha,b,c
a School of Population and Public Health, University of British Columbia, Vancouver, BC, Canada b Department of Obstetrics &
Gynaecology, University of British Columbia, Vancouver, BC, Canada c BC Children’s Hospital Research Institute, Vancouver, BC,
Canada d Department of Obstetrics and Gynaecology, King Saud University, King Khalid University Hospital, Riyadh, Saudi Arabia
e Department of Statistics, University of British Columbia, Vancouver, BC, Canada
Correspondence: G Muraca, Children’s and Women’s Hospital and Health Centre of British Columbia, C403-4500 Oak Street,
Vancouver, British Columbia, Canada, V6H 3N1. Email gmuraca@cfri.ca
Objective To quantify severe perinatal and maternal morbidity/mortality associated with mid cavity operative vaginal delivery compared with caesarean delivery.
Design Population-based, retrospective cohort study.
Setting British Columbia, Canada.
Population Term, singleton deliveries (2004–2014) by attempted mid cavity operative vaginal delivery or caesarean delivery in the second stage of labour, stratified by indication for operative delivery (n = 10 901 deliveries; 5057 indicated for dystocia, 5844 for fetal distress).
Methods Multinomial propensity scores and multivariable log-binomial regression models were used to estimate adjusted rate ratios (ARR) and 95% confidence intervals (95% CI).
The main outcome measures Composite severe perinatal morbidity/mortality (e.g. convulsions, severe birth trauma and perinatal death) and severe maternal morbidity (e.g. severe postpartum haemorrhage, shock, sepsis and cardiac complications).
Results Among deliveries with dystocia attempted mid cavity operative vaginal delivery was associated with higher rates of severe perinatal morbidity/mortality compared with caesarean delivery (forceps ARR 2.11, 95% CI 1.46–3.07; vacuum ARR 2.71, 95% CI 1.49–3.15; sequential ARR 4.68, 95% CI 3.33–6.58). Rates of severe maternal morbidity/mortality were also higher following mid cavity operative vaginal delivery (forceps ARR 1.57, 95% CI 1.05–2.36; vacuum ARR 2.29, 95% CI 1.57–3.36). Among deliveries with fetal distress, there were significant increases in severe perinatal morbidity/mortality following attempted mid cavity vacuum (ARR 1.28, 95% CI 1.04–1.61) and in severe maternal morbidity following attempted mid cavity forceps delivery (ARR 2.34, 95% CI 1.54–3.56).
Conclusion Attempted mid cavity operative vaginal delivery is associated with higher rates of severe perinatal morbidity/ mortality and severe maternal morbidity, though these effects differ by indication and instrument.
Keywords Birth injury, caesarean delivery, forceps extraction, instrumental vaginal delivery, obstetric trauma, operative vaginal delivery, vacuum extraction.
Introduction
The increased use of operative vaginal delivery has recently been advocated by the American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine as a strategy to reduce the caesarean delivery rate.1 The evaluation of approaches to achieve this end are underway2 and the current discourse surrounding operative vaginal delivery centres around methods to promote the skills required to effect such intervention.3,4 However, there is substantial uncertainty in the literature 5–11 regarding the balance of perinatal and maternal risks and benefits between operative vaginal delivery and caesarean delivery. This is at least partly because previous research has been compromised by a lack of information on the pelvic station, a key determinant of perinatal and maternal outcomes.12–14
The pelvic station is a measure of the descent of the fetal head with respect to the maternal ischial spines and operative vaginal deliveries are categorised as outlet, low or mid cavity procedures. At mid cavity station, the leading part of the fetal skull is between 0 and 2 cm below the spines, at the low cavity it is >2 cm below the ischial spines but not on the pelvic floor, and at the outlet station, the leading part of the fetal skull is on the pelvic floor and visible.12 Operative vaginal deliveries at mid cavity require the greatest operator skill and experience; consequently, it is at mid cavity station that the decision between operative vaginal delivery and caesarean delivery presents a serious challenge. Macavity operative vaginal deliveries account for up to 20% of all operative vaginal deliveries in industrialised settings and 2–3% of term, singleton deliveries overall.15 The literature on perinatal and maternal outcomes contrasting mid cavity operative vaginal delivery and caesarean delivery is based on studies undertaken 25–30 years ago 9–11 that are no longer reflective of the current obstetric practice.
We, therefore, carried out a study aimed at quantifying the effect of operative vaginal delivery at mid cavity station on perinatal and maternal morbidity and mortality compared with caesarean delivery in a cohort of women in the second stage of labour.
Methods
We conducted a population-based cohort study including all term (37–41 weeks of gestation) singletons delivered by mid cavity operative vaginal delivery or caesarean delivery in the second stage of labour, in British Columbia, Canada. Data for the study were obtained from the province’s Perinatal Data Registry. This database contains detailed demographic and clinical information on all mothers and babies in the province and is collated by trained medical record abstractors using standardised forms and coding rules. Data quality is continually assessed by means of quality and consistency checks, and information in the database has been validated16–18 and used routinely for health planning and research.19,20
The study period was restricted to fiscal years from 1 April 2004 to 31 March 2014 (hereafter referred to as years 2004–2014), when diagnoses and procedures among mothers and babies were consistently coded with the Canadian version of the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10-CA) and the Canadian Classification of Health Interventions (CCI), respectively. This included information on the stage of labour and pelvic station for all operative vaginal deliveries and the stage of labour when caesarean delivery was carried out.
Deliveries were excluded if the infant had any congenital anomaly or if the mother had a hypertensive disorder, diabetes mellitus or a placental abnormality. Further exclusions were made if the fetus was in a non-vertex presentation. Deliveries were stratified by indication for operative delivery (dystocia or fetal distress).21
Deliveries at mid cavity station were defined based on the Classification According to Station and Rotation 12 and included operative vaginal delivery by forceps, vacuum and sequential instruments in cases where the head was engaged and the leading point of the fetal skull was above the +2-cm station but below the 0-cm station. We used an intention-to-treat framework, e.g. both successful and failed forceps deliveries (followed by caesarean delivery) were included in the attempted mid cavity forceps category. Attempted mid cavity vacuum deliveries and attempted sequential instrumentation deliveries were defined in a similar manner.
The study included two primary outcomes, composite severe perinatal morbidity/mortality and composite severe maternal morbidity. Severe perinatal morbidity/mortality included convulsions, assisted ventilation by endotracheal intubation, 5-minute Apgar score <4, severe birth trauma (intracranial haemorrhage, skull fracture, severe injury to the central or peripheral nervous systems, long bone injury, subaponeurotic haemorrhage, and injury to liver or spleen), stillbirth and neonatal death. Severe maternal morbidity included severe postpartum haemorrhage (requiring transfusion), shock, sepsis, obstetric embolism, cardiac complications and acute renal failure. Secondary outcomes included respiratory distress in the infant (including hyaline membrane disease, idiopathic respiratory distress syndrome, transient tachypnoea of the newborn and other neonatal respiratory distress), postpartum haemorrhage, as well as birth and obstetric trauma. Birth trauma included intracranial haemorrhage, injury to the central or peripheral nervous systems, injury to the scalp or the skeleton, and other birth injuries. Obstetric trauma included severe perineal lacerations (third- and fourth-degree), cervical and high vaginal laceration, pelvic haematoma, obstetric injury to the pelvic organs, pelvic joints or ligaments, and other obstetric trauma. The inclusion and exclusion criteria, indications for operative delivery, confounders and outcomes of interest along with the associated ICD-10-CA and CCI codes used in the study are listed in the Supporting information (Table S1).
The effect of mid cavity operative vaginal delivery was quantified using two approaches, namely, confounder adjustment using propensity score methods and multivariable regression. Although regression methods are commonly used to adjust for confounding factors in non-experimental studies, propensity score analysis has recently gained traction especially in studies involving rare outcomes. Propensity score analysis involves a two-step procedure in which the propensity for a subject to have received an intervention (mid cavity operative vaginal or caesarean delivery) is first quantified based on their confounder patterns. Adjustment for this propensity score is carried out through a second step that effectively eliminates bias due to associations between the determinant being studied (mid cavity operative vaginal delivery) and the confounding factors.
We used multinomial propensity scores to estimate the probability that a woman would have delivered by mid cavity forceps, mid cavity vacuum, sequential mid cavity instrumentation or caesarean delivery is given her covariate pattern after stratifying by indication (dystocia or fetal distress). The confounders included in the propensity score were maternal age (<20, 20–24, 25–29, 30–34, 35–39, ≥40 years), parity (0, ≥1), prepregnancy weight (kg), previous caesarean delivery (Y/N), the position of the fetal head at delivery (occiput anterior versus occiput posterior/transverse), birthweight (<3000, 3000–3499, 3500– 3999, 4000–4499, ≥4500 g), income quintile (a household size-adjusted measure of household income; lower values represent lower income) and year of birth. All possible two-way interactions were included in the propensity score estimation. We used the Toolkit for Weighting and Analysis of Nonequivalent Groups (TWANG) package to estimate the propensity scores and weights by implementing generalised boosted regression models.22 Box plots were used to assess overlap between the weighted mode of delivery groups. We then used log-binomial regression to regress our composite perinatal and maternal outcomes against indicator variables denoting mode of delivery in the weighted sample. Adjusted rate ratios (ARR) and 95% confidence intervals (CI) were obtained.
In addition, we modelled the same associations using (1) logistic regression adjusting for the same eight covariates listed above and (2) multivariable logistic regression with propensity score weighting and including the same eight covariates that were included in the propensity score to obtain doubly robust estimators. These estimates were interpreted as ARRs since the outcomes were rare. Modification of the effect of mode of delivery on perinatal and maternal morbidity/mortality by the position of the fetal head at delivery (occiput anterior versus occiput posterior/transverse) and by a diagnosis of the prolonged second stage of labour (ICD-10 CA O631, yes/no) was examined by introducing interaction terms into the regression models. Missing values for the prepregnancy weight (15%), the position of the fetal head at delivery (29%) and income quintile (1.5%) were addressed with multiple imputations using the fully conditional method to create ten imputed data sets. The discriminant function method was used to impute values for categorical variables and linear regression was used for continuous variables.23 Lastly, the magnitude of absolute effects was quantified by calculating adjusted rate differences and the adjusted number-needed-to-treat (NNT). The adjusted NNTs represent the number of women delivered by operative vaginal delivery that would have had to be delivered by caesarean to avoid one case of the outcome of interest. All analyses were carried out using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). The study was approved by the University of British Columbia’s Clinical Research Ethics Board (H12-0277).
Patient involvement
Patients were not involved in the development or design of this study.
Results
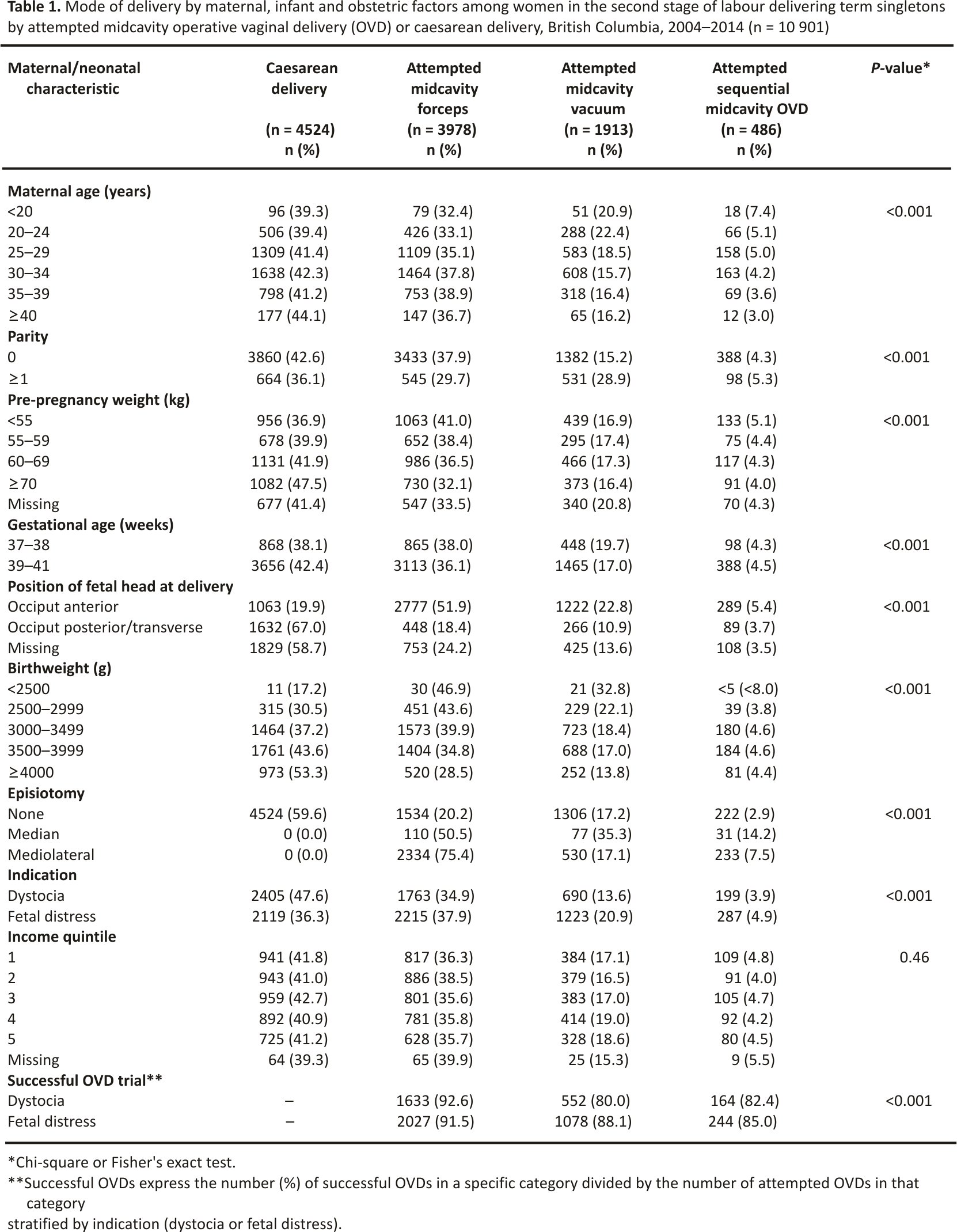
The study population included 10 901 deliveries; 5057 attempted mid cavity operative vaginal or caesarean deliveries with dystocia and 5844 attempted mid cavity operative vaginal or caesarean deliveries with fetal distress (see Supporting information, Figure S1). The rate of severe perinatal morbidity/ mortality was 1.42% and 2.34% in the dystocia and fetal distress groups, respectively. The rate of severe maternal morbidity was 1.03% in both groups. Nulliparous women, older women (≥35 years), women with higher prepregnancy weight (≥70 kg) and those who delivered at later gestational ages were more likely to have had a caesarean delivery (Table 1). Attempted mid cavity forceps was more commonly used in nulliparous women compared with attempted mid cavity vacuum, whereas the reverse was true among multiparous women. Attempted operative vaginal delivery was more common in deliveries with babies of lower birth weight, whereas caesarean delivery was more frequent in macrosomic infants (≥4000 g). Women with dystocia had higher rates of caesarean delivery compared with women who had fetal distress. Operative vaginal delivery was more likely to be successful following forceps attempts (92.6% and 91.5% among women with dystocia and fetal distress, respectively) than following vacuum extraction attempts (80.0% and 88.1%, respectively; Table 1). Propensity score weighting converged and achieved a good balance in the mode of delivery groups; the overlap of propensity scores in the weighted groups was satisfactory in both the dystocia and fetal distress cohorts (see Supporting information, Figures S2, S3, S4 and S5).
Severe perinatal morbidity/mortality
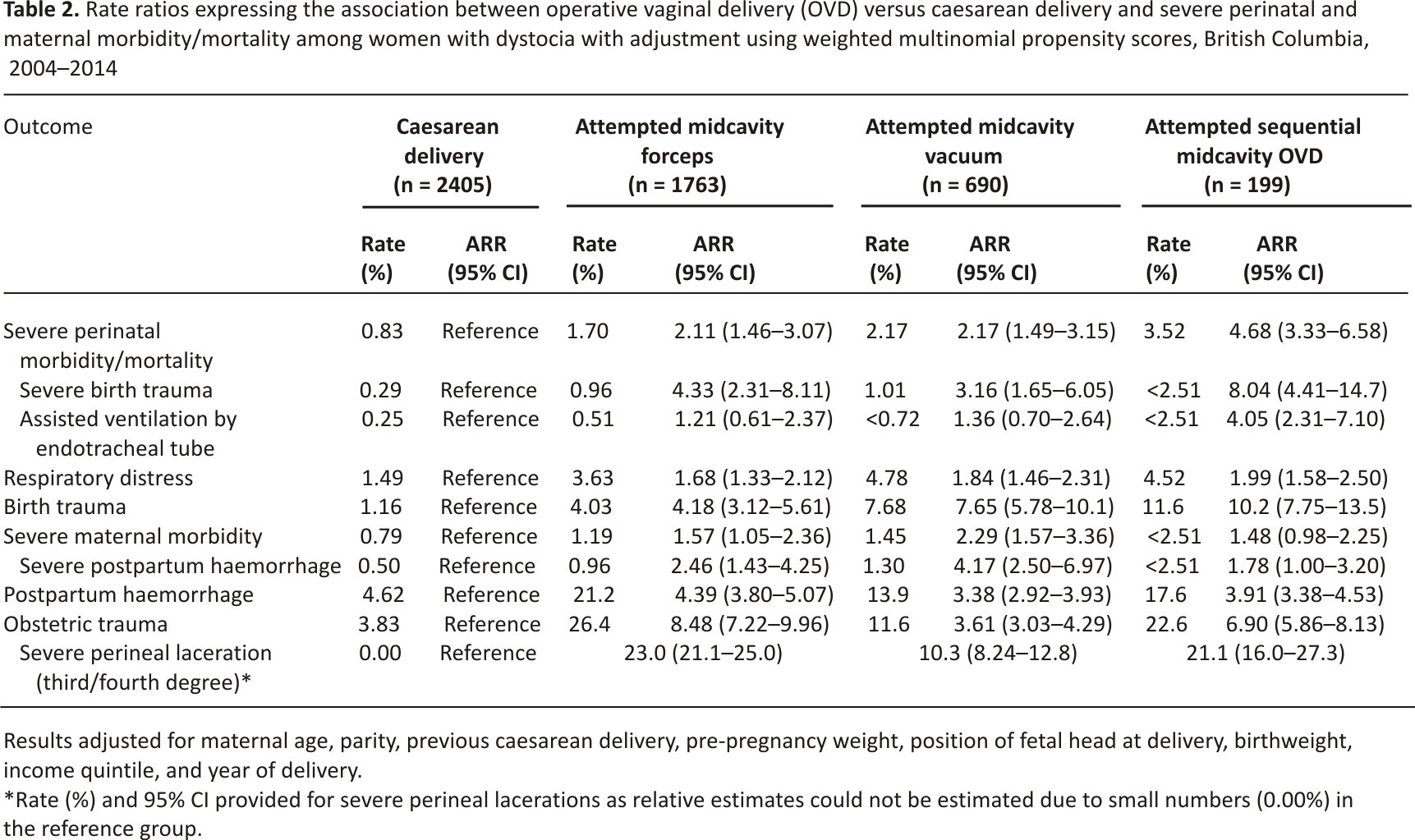
Among deliveries with dystocia, attempted mid cavity operative vaginal delivery was associated with higher rates of severe perinatal morbidity/mortality compared with caesarean delivery (forceps 1.7%, vacuum 2.2%, sequential 3.5% and caesarean 0.8%; forceps ARR 2.11, 95% CI 1.46–3.07, vacuum ARR 2.17, 95% CI 1.49–3.15, sequential ARR 4.68, 95% CI 3.33–6.58; Table 2). Rates of severe birth trauma were similarly higher in attempted forceps deliveries (1.0%; ARR 4.33, 95% CI 2.31–8.11) and attempted vacuum deliveries (1.0%; ARR 3.16, 95% CI 1.65–6.05) compared with caesarean delivery (0.3%). Sequential mid cavity instrument use was associated with the highest rates of severe birth trauma (ARR 8.04, 95% CI 4.41–14.7) and any birth trauma (11.6% versus 1.2% in caesarean deliveries; ARR 10.2, 95% CI 7.75–13.5; Table 2). Attempted mid cavity forceps and vacuum deliveries were also associated with significantly higher rates of respiratory distress and all birth trauma (Table 2 and see Supporting information, Table S2).
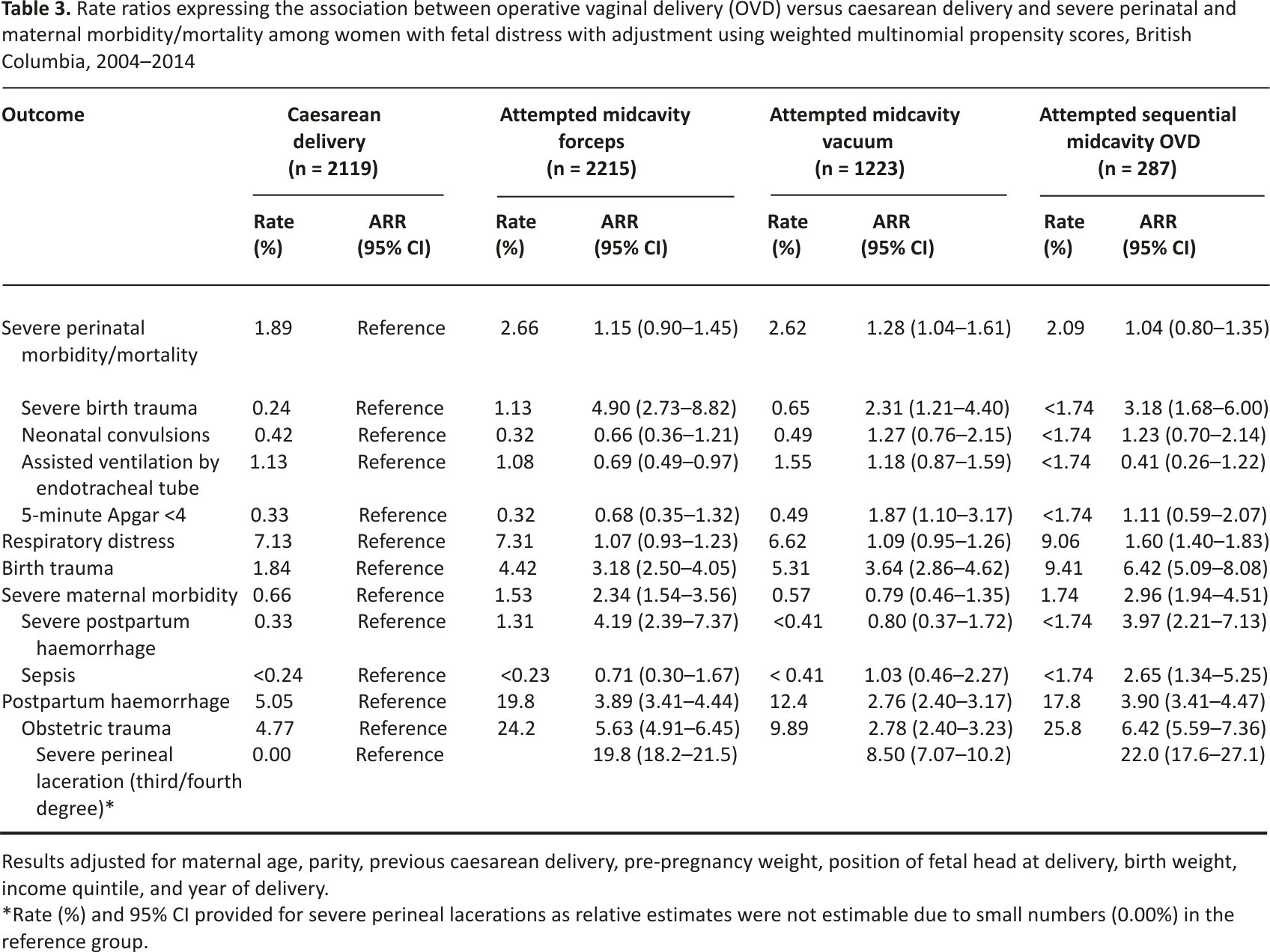
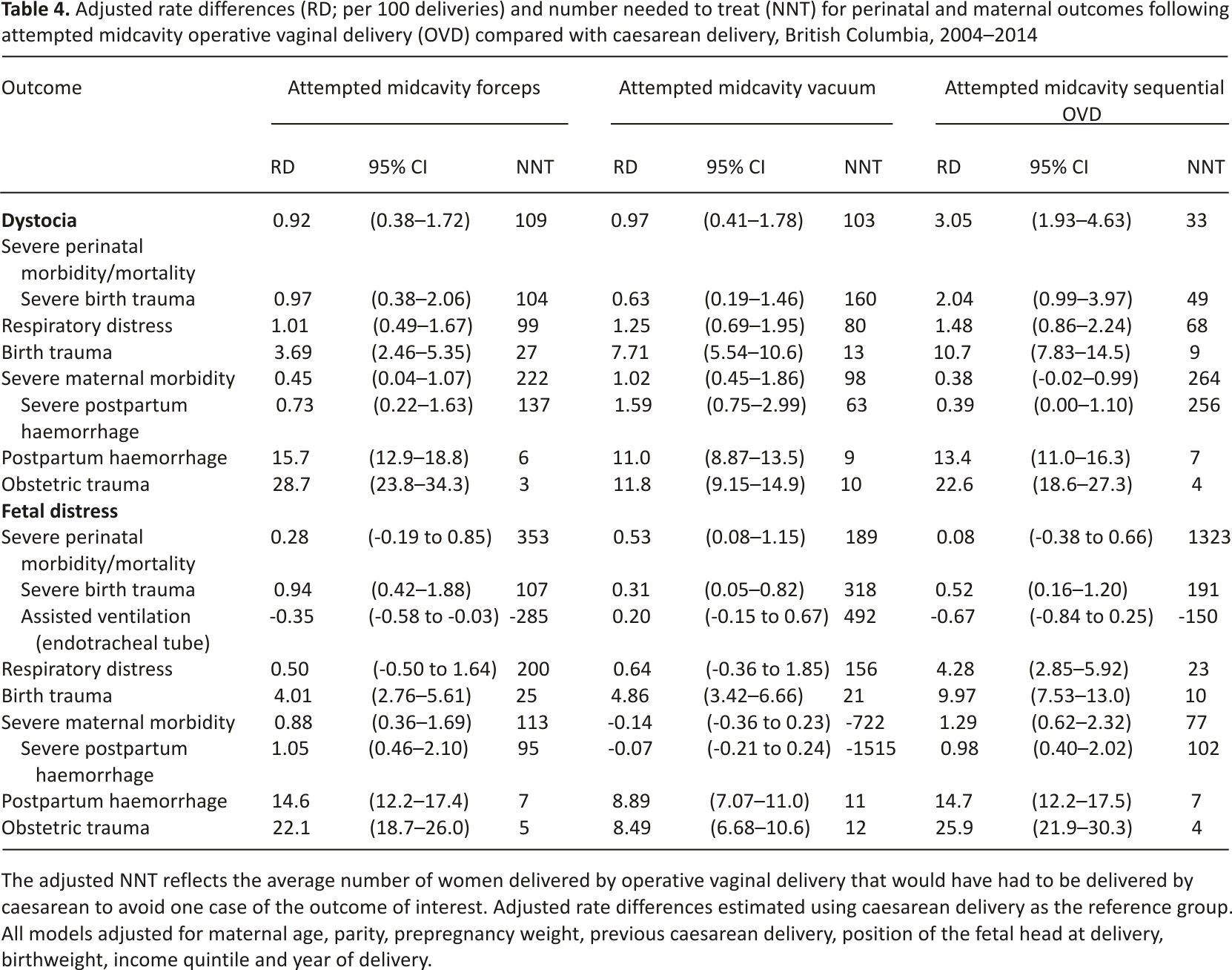
Among deliveries with fetal distress, the rate of severe perinatal morbidity/ mortality was similar in the attempted mid cavity forceps, sequential instrument and caesarean delivery groups. However, it was significantly higher in the attempted mid cavity vacuum group (2.6% versus 1.9% in the caesarean group; ARR 1.28, 95% CI 1.04–1.61; Table 3 and see Supporting information, Table S2). Severe birth trauma rates were higher in all the attempted mid cavity operative vaginal delivery group (forceps 1.1%; ARR 4.90, 95% CI 2.73–8.82; vacuum 0.7%; ARR 2.31, 95% CI 1.21–4.40; sequential <1.7%; ARR 3.18, 95% CI 1.68–6.00) compared with the caesarean delivery group (0.2%). The rate of assisted ventilation by endotracheal tube was significantly lower among attempted mid cavity forceps deliveries compared with caesarean delivery (ARR 0.69, 95% CI 0.49–0.97). The rate of any birth trauma was higher in all operative vaginal delivery categories (forceps 4.4% versus 1.8% following caesarean delivery; ARR 3.18, 95% CI 2.50–4.05; vacuum 5.3%; ARR 3.64, 95% CI 2.86–4.62; sequential 9.4%; ARR 6.42, 95% CI 5.09–8.08). Adjusted rate differences, 95% CIs, and adjusted NNTs are listed in Table 4; NNT for severe perinatal morbidity/mortality was 109 for mid cavity forceps, 103 for mid cavity vacuum and 33 for sequential instrumentation in deliveries with dystocia.
Severe maternal morbidity
Rates of severe maternal morbidity were higher following mid cavity operative vaginal delivery compared with caesarean delivery in the dystocia group (1.2% and 1.5% following forceps and vacuum, respectively compared with 0.8% following caesarean delivery; forceps ARR 1.57, 95% CI 1.05–2.36; vacuum ARR 2.29, 95% CI 1.57–3.36); Table 2 and see Supporting information, Table S2). In deliveries with fetal distress, rates of maternal morbidity were increased following attempted mid cavity forceps (1.5% versus 0.7% in caesarean delivery; ARR 2.34, 95% CI 1.54–3.56) and sequential operative vaginal delivery (1.7%; ARR 2.96, 95% CI 1.94–4.51; Table 3). This higher maternal morbidity was mainly due to higher rates of severe postpartum haemorrhage in the mid cavity forceps group (1.3% versus 0.3%; ARR 4.19, 95% CI 2.39–7.37). In women with dystocia, the ARR for severe postpartum haemorrhage among women delivered by mid cavity forceps was 2.46 (95% CI 1.43–4.25), whereas the same ARR was 4.17 (95% CI 2.50–6.97) for women delivered by vacuum (Table 2).
Obstetric trauma
Obstetric trauma rates were high following attempted vacuum delivery (11.6% versus 3.8% following caesarean deliveries; ARR 3.61, 95% CI 3.03–4.29; Table 2 and see Supporting information, Table S2) and highest following attempted mid cavity forceps delivery (26.4% versus 3.8%; ARR 8.48, 95% CI 7.22–9.96) among women with dystocia. Obstetric trauma rates among deliveries with fetal distress were similar (Table 3 and see Supporting information, Table S2). Severe perineal laceration rates were high among attempted mid cavity operative vaginal deliveries, ranging from 8.5% following attempted vacuum deliveries for fetal distress to 23.0% among attempted forceps deliveries for dystocia (see Supporting information, Figures S6 and S7). NT for obstetric trauma was three for mid cavity forceps, ten for mid cavity vacuum and four for sequential instrumentation among women with dystocia (Table 4).
Sensitivity analyses and effect modification
The associations between attempted mid cavity operative vaginal delivery and severe perinatal and maternal morbidity/ mortality were similar when a multivariable logistic regression model was used although the confidence intervals were wider in the logistic regression model (see Supporting information, Table S3). The model using propensity score weights and doubly robust estimators also produced similar estimates although the ARRs were attenuated in the log-binomial model with propensity score weighting alone (see Supporting information, Table S4). The estimates from the data with multiple imputations were very similar to the complete case estimates. The association between attempted mid cavity vacuum delivery and severe perinatal morbidity/ mortality was modified by the position of the fetal head at delivery among deliveries with fetal distress (ARR for deliveries with fetal head in the occiput anterior position 0.97 (95% CI 0.48–1.96), ARR in deliveries with fetal head in occiput posterior position 3.00 (95% CI 1.28–7.01, P-value for interaction 0.03; see Supporting information, Table S5).
The association between attempted mid cavity operative vaginal delivery and severe perinatal morbidity/mortality was similar among women with and without a prolonged second stage of labour (see Supporting information, Tables S6 and S7). However, the association between attempted mid cavity forceps and severe maternal morbidity was modified by the duration of the second stage among deliveries with fetal distress (ARR without prolonged second stage 5.58, 95% CI 1.94–16.1, ARR with prolonged second stage 0.86, 95% CI 0.32–2.29, P-value for interaction 0.003; see Supporting information, Table S7). The prolonged second stage similarly attenuated the association between attempted mid cavity forceps delivery and respiratory distress and obstetric trauma among women with dystocia and between attempted mid cavity vacuum delivery and postpartum haemorrhage among deliveries with fetal distress.
Discussion
Main findings
Our study showed that among term singleton deliveries in the second stage of labour, attempted mid cavity operative vaginal delivery was associated with an increased risk of severe perinatal morbidity/mortality compared with caesarean delivery. The magnitude of the increased risk varied by indication for delivery, being significantly larger in the dystocia group relative to the fetal distress group. This difference in the effect of attempted operative vaginal delivery by indication appears to reflect the greater fetal jeopardy associated with fetal distress and the consequent higher baseline rate of adverse outcomes even in the caesarean delivery group. We also found a substantially greater risk of birth and obstetric trauma following operative vaginal delivery compared with caesarean delivery, with 2.8- to 8.5-fold higher rates depending on indication and instrument. Composite severe maternal morbidity rates were higher among operative vaginal delivery groups compared with the caesarean delivery group except for mid cavity vacuum deliveries among women with fetal distress.
Strengths and limitations
The strengths of our data source and analysis include an ability to identify operative vaginal deliveries at mid cavity station and to restrict our caesarean delivery cohort to women in the second stage of labour. Women who had a failed operative vaginal delivery (and eventually delivered by caesarean) were included in the operative vaginal delivery group. This ensured a clinically appropriate comparison of the different modes of delivery using an intention-to-treat framework. We used propensity score analysis, which has advantages over regression analysis estimates in specific situations,24–27 although in this instance the findings were similar to results from multivariable regression.
The limitations of our study include its non-experimental design. Although we used state-of-the-art propensity score analysis and multivariable regression methods to control for confounding, such methods cannot address imbalances between groups due to unmeasured confounders. On the other hand, the feasibility of conducting randomised trials for assessing the safety of mid cavity operative vaginal delivery is questionable. More importantly, non-experimental evaluation of the unintended effects of mid cavity vacuum and forceps delivery on maternal and perinatal severe morbidity (such as obstetric and birth trauma) is not likely to be compromised by confounding by indication (which biases estimates of the intended effect).28 The inability to account for the skill of the operator is another potential limitation; the findings of our study may not be applicable to practitioners with proficiency and expertise in mid cavity operative vaginal delivery. Nevertheless, our study quantifies the effect of the average contemporary practitioner in Canada and this is relevant for women in labour who have a limited ability to assess their provider’s expertise in mid cavity operative vaginal delivery. Another limitation relates to the determination of pelvic station, which can be challenging per se and can be affected by moulding and fetal head position.29,30 Our study findings reflect the average safety of mid cavity operative vaginal delivery as carried out under current norms of diagnosis and available expertise. Although we restricted caesarean deliveries to those carried out in the second stage of labour, we were constrained by our inability to ascertain information on pelvic station for caesarean deliveries. However, only a small fraction of caesarean deliveries would have been carried out with the fetal head above the mid cavity station.31 On the other hand, our estimates of the adverse effects of mid cavity operative vaginal delivery may have been underestimated as some caesarean deliveries in the second stage of labour would have been carried out with the fetal head below mid cavity station.32,33 Further limitations of our data source included the absence of information on the use of rotational forceps and missing information on a significant fraction of subjects for variables such as prepregnancy weight and position of the fetal head, which was addressed using multiple imputations. We were also unable to assess the long-term effects of caesarean delivery and mid cavity operative vaginal delivery.
Interpretation
The increase in severe maternal morbidity following mid cavity forceps delivery was primarily due to the increased rate of severe postpartum haemorrhage. Higher rates of severe postpartum haemorrhage were also found in mid cavity vacuum deliveries among women with dystocia. Increased rates of postpartum haemorrhage following vacuum delivery at low and outlet station has been reported previously, 34 although such reports were restricted to babies with birth weight ≥4000 g. Studies that have compared postpartum haemorrhage in mid cavity operative vaginal deliveries and caesarean deliveries have yielded conflicting results8,9,35,36 at least partly due to differences in definitions of postpartum haemorrhage. We defined severe postpartum haemorrhage as postpartum haemorrhage requiring transfusion to ensure a clinically meaningful and standardised outcome. Although cases of postpartum haemorrhage observed in our study were due to atonic postpartum haemorrhage, the high rates of obstetric trauma following mid cavity operative vaginal delivery in our study suggest that some proportion of such haemorrhage was due to cervical, vaginal and perineal trauma.37
Third- and fourth-degree perineal laceration rates in our study were high following midcavity operative vaginal delivery. Similar high rates have been reported in other recent studies of operative vaginal delivery.13,31 Validation studies18 show that the diagnosis of third- and fourth-degree perineal lacerations in Canadian hospitalisation data is accurate (sensitivity and specificity of 97.1% and 99.9%, respectively, for third-degree, and 94.7% and 99.9%, respectively, for fourth-degree tears). With rates of obstetric anal sphincter injury as high as 23.0% following attempted mid cavity forceps deliveries, it is imperative that the risks and relevant long-term quality-of-life implications for pelvic floor health of attempted mid cavity operative vaginal delivery be discussed with women both in the antenatal period, as well as during labour (as currently done with regard to the surgical risks associated with caesarean delivery).
Conclusion
Attempted midcavity operative vaginal delivery is associated with substantially higher rates of severe birth trauma and obstetric trauma. Rates of severe perinatal and maternal morbidity/mortality following midcavity operative vaginal delivery are also increased, though these associations vary by indication and instrument used. The retrospective nature of our analysis limits our ability to make causal inferences based on these results and carefully designed prospective studies examining this issue are warranted. Nevertheless, our results suggest that encouraging higher rates of operative vaginal delivery as a strategy to reduce the caesarean delivery rate could result in increases in severe perinatal and maternal morbidity, especially birth trauma, severe postpartum haemorrhage and obstetric trauma.
Disclosure of interest
None declared. Completed disclosure of interests forms available to view online as Supporting Information.
Contribution to authorship
GMM and KSJ proposed the study concept and design and were assisted by AS, SL, YS, RB and GWC. GMM acquired the data and carried out the analyses. AS, SL, YS, RB, GWC and KSJ reviewed the preliminary and final analyses. GMM drafted the manuscript and AS, SL, YS, RB, GWC and KSJ provided critical input in connection with the intellectual content. All authors approved the final version of the manuscript.
Details of ethics approval
The study was approved on 3 December 2012 by the University of British Columbia’s Clinical Research Ethics Board (H12-0277).
Funding
GMM is the recipient of a Vanier Canada Graduate Scholarship; KSJ is supported by the BC Children’s Hospital Research Institute and holds a Canadian Institutes of Health Research (CIHR) Chair in maternal, fetal and infant health services research (APR-126338). This study was funded by a CIHR grant on severe maternal morbidity (MAH-15445). The funding source has no direct role in the study design; collection, analysis or interpretation of data; the writing of the report or the decision to submit.
Acknowledgements
Data for this study were provided by the Perinatal Services British Columbia (PSBC); however, the analyses, conclusions, and opinions expressed herein are those of the authors and not those of PSBC.
Supporting Information
Additional Supporting Information may be found in the online version of this article:
Figure S1. Derivation of the study cohort.
Figure S2. Propensity score unweighted and weighted effect size plots for the dystocia cohort.
Figure S3. Propensity score unweighted and weighted effect size plots for the fetal distress cohort.
Figure S4. Propensity score overlap assessment by mode of delivery in the dystocia cohort.
Figure S5. Propensity score overlap assessment by mode of delivery in the fetal distress cohort.
Figure S6. Rates (per 100 deliveries) and 95% confidence intervals of third and fourth-degree perineal lacerations following midcavity operative vaginal delivery by instrument, indication, and type of episiotomy, British Columbia, 2004–2014.
Figure S7. Rates (per 100 deliveries) and 95% confidence intervals of third and fourth-degree perineal lacerations following midcavity operative vaginal delivery by instrument and indication, British Columbia, 2004–2014.
Table S1. International Classification of Diseases and Related Health Problems Tenth Revision, Canadian version (ICD-10-CA), and Canadian Classification of Health Interventions (CCI) codes used for population selection and to classify determinants, outcomes, and confounders.
Table S2. Numbers and rates of all components of perinatal and maternal outcomes by attempted mode of delivery, British Columbia, 2004–2014.
Table S3. Rate ratios expressing the association between operative vaginal delivery (OVD) versus caesarean delivery and severe perinatal and maternal morbidity/mortality among women with dystocia and fetal distress with adjustment using multivariable logistic regression, British Columbia, 2004– 2014.
Table S4. Rate ratios expressing the association between operative vaginal delivery (OVD) versus caesarean delivery and severe perinatal and maternal morbidity/mortality among women with dystocia and fetal distress with adjustment using regression with propensity score weights and doubly robust estimators, British Columbia, 2004–2014.
Table S5. Adjusted rate ratios (ARR) and 95% confidence intervals (CI) for severe perinatal and maternal composite morbidity and mortality following deliveries by attempted midcavity operative vaginal delivery compared with caesarean delivery, stratified by the position of the fetal head at delivery, British Columbia, 2004–2014.
Table S6. Adjusted rate ratios (ARR) and 95% confidence intervals (CI) for perinatal and maternal outcomes following deliveries with dystocia by attempted midcavity operative vaginal delivery compared with caesarean delivery, stratified by the prolonged second stage of labour, British Columbia, 2004–2014.
Table S7. Adjusted rate ratios (ARR) and 95% confidence intervals (CI) for perinatal and maternal outcomes following deliveries with fetal distress by attempted midcavity operative vaginal delivery compared with caesarean delivery, stratified by the prolonged second stage of labour, British Columbia, 2004–2014.
References
1 Caughey AB, Cahill AG, Guise J-M, Rouse DJ. Safe prevention of the primary cesarean delivery. Am J Obstet Gynecol 2014;210:17–93.
2 Gossett DR, Gilchrist-Scott D, Wayne DB, Gerber SE. Simulation training for forceps-assisted vaginal delivery and rates of maternal perineal trauma. Obstet Gynecol 2016;128:429–35.
3 Deering S. Forceps, simulation, and social media. Obstet Gynecol 2016; 128:425–6.
4 Dildy GA, Belfort MA, Clark SL. Obstetric forceps: a species on the brink of extinction. Obstet Gynecol 2016;128: 436–9.
5 Towner D, Castro MA, Eby-Wilkens E, Gilbert WM. Effect of mode of delivery in nulliparous women on the neonatal intracranial injury. N Engl J Med 1999; 341:1709–14.
6 Walsh CA, Robson M, McAuliffe FM. Mode of delivery at term and adverse neonatal outcomes. Obstet Gynecol 2013;121:122–8.
7 Werner EF, Janevic TM, Illuzzi J, Funai EF, Savitz DA, Lipkind HS. Mode of delivery in nulliparous women and neonatal intracranial injury. Obstet Gynecol 2011;118:1239–46.
8 Murphy DJ, Liebling RE, Verity L, Swingler R, Patel R. Early maternal and neonatal morbidity associated with operative delivery in the second stage of labour: a cohort study. Lancet 2001;358: 1203–7.
9 Robertson PA, Laros RK Jr, Zhao R-L. The neonatal and maternal outcome in low-pelvic and mid pelvic operative deliveries. Am J Obstet Gynecol 1990;162:1436–44.
10 Bashore RA, Phillips WH Jr, Brinkman CR 3rd. A comparison of the morbidity of mid forceps and cesarean delivery. Am J Obstet Gynecol 1990;162: 1428–34.
11 Dierker LJ, Rosen MG, Thompson K, Debanne S, Linn P. The mid forceps: maternal and neonatal outcomes. Am J Obstet Gynecol 1985;152: 176–83.
12 Cunningham FG, Leveno KJ, Bloom SL, Spong CY, Dashe J. Operative vaginal delivery. In: Cunningham FG, Leveno KJ, Bloom SL, Spong CY, Dashe J, editors. Williams Obstetrics, 24th edn. New York, NY: McGraw-Hill Education, 2013. [http://access medicine. mhmedical.com/content. aspx?bookid=1057&Sectionid=59789170]. Accessed 25 February 2017.
13 Halscott TL, Reddy UM, Landy HJ, Ramsey PS, Iqbal SN, Huang C, et al. Maternal and neonatal outcomes by attempted mode of operative delivery from a low station in the second stage of labor. Obstet Gynecol 2015;126: 1265–72.
14 Bailit J, Garrett J. Comparison of risk-adjustment methodologies for cesarean delivery rates. Obstet Gynecol 2003;102:45–51.
15 Muraca GM, Sabr Y, Brant R, Cundiff GW, Joseph KS. Temporal and regional variations in operative vaginal delivery in Canada by pelvic station, 2004–2012. J Obstet Gynaecol Can 2016;38:627–35.
16 Frosst G, Hutcheon J, Joseph KS, Kinniburgh B, Johnson C, Lee L. Validating the British Columbia Perinatal Data Registry: a chart reabstraction study. BMC Pregnancy Childbirth 2015;15:123.
17 Frosst G. Validity of pre-pregnancy body mass index (BMI) information derived from a population-based perinatal database. Healthy Mothers and Healthy Babies: New Research and Best Practice Conference 2014. Vancouver, British Columbia.
18 Joseph KS, Fahey J. Validation of perinatal data in the Discharge Abstract Database of the Canadian Institute for Health Information. Chronic Dis Can 2009;29:96–100.
19 Perinatal Services British Columbia. Perinatal health report: deliveries in British Columbia 2014/15. 2016. Vancouver, BC. [http://www.peri natalservicesbc.ca/Documents/Data-Surveillance/Reports/PHR/PHR_BC_2014_15.pdf]. Accessed 25 February 2016.
20 Perinatal Services British Columbia. Surveillance perinatal indicators annual report: British Columbia residents delivering in British Columbia. 2016. Vancouver, BC. [http://www.perinatalservicesbc.ca/Documents/Data-Surveillance/Indicators/Annual/AnnualIndicatorsResidence _2013_14_BC.pdf]. Accessed 25 February 2016.
21 Henry OA, Gregory KD, Hobel CJ, Platt LD. Using ICD-9 codes to identify indications for primary and repeat cesarean sections: agreement with clinical records. Am J Public Health 1995;85:1143–6.
22 McCaffrey DF, Griffin BA, Almirall D, Slaughter ME, Ramchand R, Burgette LF. A tutorial on propensity score estimation for multiple treatments using generalized boosted models. Stat Med 2013;32:3388–414.
23 Lee KJ, Carlin JB. Multiple Imputation for missing data: fully conditional specification versus multivariate normal imputation. Am J Epidemiol 2010;171:624–32.
24 Harder VS, Stuart EA, Anthony J. Propensity score techniques and the assessment of measured covariate balance to test causal association in psychological research. Psychol Methods 2010;15:234–49.
25 Lee BK, Lessler J, Stuart E. Improving propensity score weighting using machine learning. Stat Med 2010;29: 337–46.
26 Lee BK, Lessler J, Stuart E. Weight trimming and propensity score weighting. PLoS ONE 2011;6:e18174.
27 Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar Behav Res 2011;46:399–424.
28 Joseph KS, Mehrabadi A, Lisonkova S. Confounding by indication and related concepts. Curr Epidemiol Rep 2014;1:1v8.
29 Knight D, Newnham JP, McKenna M, Evans S. Comparison of abdominal and vaginal examinations for the diagnosis of engagement of the fetal head. Aust N Z J Obstet Gynaecol 1993;33:154–8.
30 Dupuis O, Silveira R, Zentner A, Dittmar A, Gaucherand P, Cucherat M, et al. Birth simulator: reliability of transvaginal assessment of fetal head station as defined by the American College of Obstetricians and Gynecologists classification. Am J Obstet Gynecol 2005;192:868–74.
31 Dupuis O, Ruimark S, Corinne D, Simone T, Andr_e D, Ren_e-Charles R. Fetal head position during the second stage of labour: comparison of digital vaginal examination and transabdominal ultrasonographic examination. Eur J Obstet Gynaecol Reprod Biol 2005;123:193–7.
32 Tan J. Difficult caesarean delivery of an impacted head and neonatal skull fracture. Can the morbidity be avoided? Obstet Gynecol 2007;27: 427–8.
33 Steer PJ. Is a fractured skull discovered in the neonate after caesarean section delivery always evidence of negligence? BJOG 2016;123:336.
34 Bailit JL, Grobman WA, Rice MM, Wapner RJ, Reddy UM, Varner MW, et al. Evaluation of delivery options for second-stage events. Am J Obstet Gynecol 2016;214(638):e1–10.
35 Lowe B. Fear of failure: a place for the trial of instrumental delivery. BJOG 1987;94:60–6.
36 Murphy D. Cohort study of operative delivery in the second stage of labour and standard of obstetric care. BJOG 2003;110:610–5.
37 Knight M, Callaghan WM, Berg C, Alexander S, Bouvier-Colle MH, Ford JB, et al. Trends in postpartum haemorrhage in high resource countries: a review and recommendations from the International Postpartum Hemorrhage Collaborative Group. BMC Pregnancy Childbirth 2009;9:55.
Credits: Muraca GM, Skoll A, Lisonkova S, Sabr Y, Brant R, Cundiff GW, Joseph KS. Perinatal and maternal morbidity and mortality among term singletons following midcavity operative vaginal delivery versus caesarean delivery. BJOG. 2018 May; 125(6):693-702. Epub 2017 Aug 21.






