

1Massimo Giusti & 2Marilena Sidoti
Endocrine Unit, Centro Clinico Diagnostico Priamar, Via dei Partigiani 13R, Savona, 17100, Italy Dipartimento di Medicina Interna, Università di Genova, Genoa, Italy
2Endocrine Unit, Centro Clinico Diagnostico Priamar, Via dei Partigiani 13R, Savona, 17100, Italy Endocrine Unit, Azienda Sanitaria Locale 2 Savonese, Savona, Italy
Abstract
Background
TSH is the primary test for assessing thyroid function, and the normal TSH references provided by manufacturers are typically used in diagnosis. In the age of gender medicine, however, there is a need to refine normal TSH ranges.
Aim
This study aimed to construct a normal TSH range in women living in our district. The data were collected in a secondary-level centre located in Savona (Liguria, Italy).
Methods
From 2003 to 2022, 6227 medical records from women undergoing their first endocrinological examination were anonymously evaluated. After the application of exclusion criteria, statistical analysis was performed anonymously on a sample of 2,597 medical records.
Results
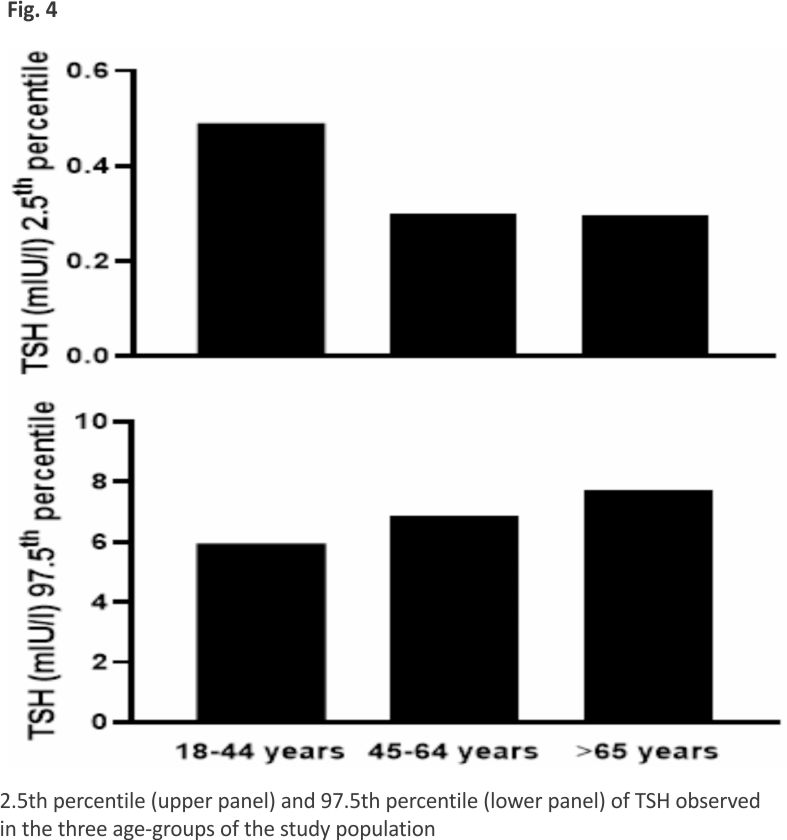
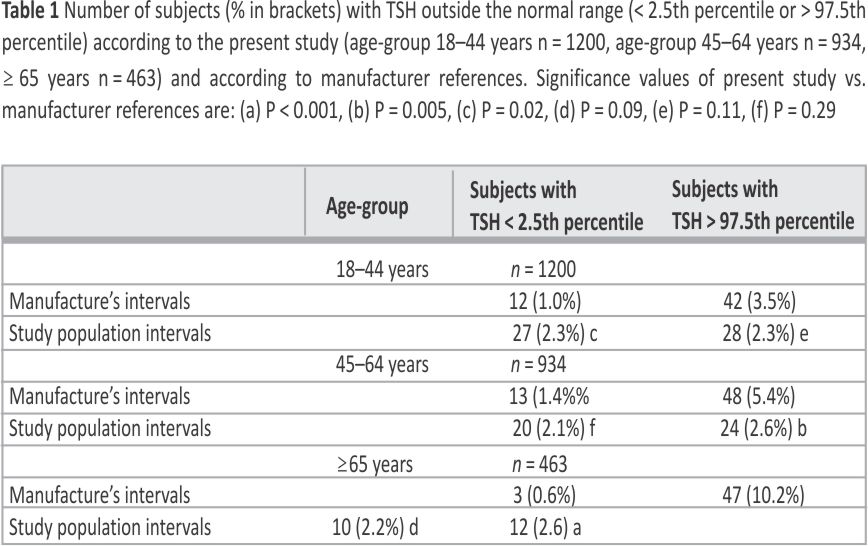
The pooled median 2.5th and 97.5th percentiles of TSH provided by manufacturers were 0.20 mIU/l and 5.64 mIU/l, respectively. In the study population, median (2.5th-97.5th percentiles) TSH was 1.70 mIU/l (0.37–6.95 mIU/l). TSH and patient age did not vary significantly over the years (2003–2022). A slight negative correlation was found between TSH and age (P = 0.05). On stratifying the sample into three age-groups (18–44 years, N = 1200; 45–64 years N = 934; ≥65 years, N = 463), TSH was 1.75 mIU/l (0.49–5.94 mIU/l), 1.70 mIU/l (0.30–6.89 mIU/l) and 1.64 mIU/l (0.30–7.69 mIU/l), respectively. When TSH was evaluated according to the age-related range instead of the pooled range reported by manufacturers, the number of women aged 18–44 years considered to have sub-clinical hyperthyroidism increased slightly (P = 0.02) and the number of women in the 45-64-year and ≥65-year age-groups considered to have sub-clinical hypothyroidism decreased signifi- cantly (P = 0.05 and P < 0.001).
Conclusions
This is the first study in Liguria to establish new age-specific reference values for TSH in women. Based on a large number of data, this new age-related range could be more extensively employed to improve diagnosis. The main result of implementing age-related normal TSH levels between the 2.5th and 97.5th percentiles seems to be both a slight increase in 18-44-year-old women and a significant reduction in > 45-year-old women in whom sub-clinical hyperthyroidism or hypothyroidism, respectively, should be promptly treated.
Introduction
Thyroid-stimulating hormone (TSH) is the key indicator of thyroid function. Several factors can affect TSH in adults (heredity, ethnicity, iodine status, body weight, smoking status, concomitant diseases, drugs, autoimmunity, time of sampling, sex and age) 1. Available assay methods and reference ranges influence TSH evaluation. The American Thyroid Association, in its centennial article, reports technical advances in laboratory thyroid tests in the last seven decades, with the third-generation TSH assay being available on most automated instrument platforms 2. Moreover, despite improvements in functional sensitivity and the use of the same standard, TSH assays differ in their specificity, and the manufacturers’ reference ranges are somewhat different 2. In addition, inter-method differences, TSH isoforms or TSH antibodies and several sources of interference in assays can contribute to diagnostic errors1,2.
Normal TSH ranges provided by manufacturers do not consider possible gender and age differences, except for the occasional specification of trimester-specific TSH ranges in pregnancy. Current guidelines on laboratory medicine recommend that each clinical analysis laboratory should establish its reference intervals according to the characteristics of the local population. Reference limits can be obtained from strictly healthy individuals (direct method), with a minimum of 120 reference individuals being required in order to determine the reference interval of an analyte; this would represent approximately 95% of the values found in the given population 3. In routine practice, however, the direct method is hard to apply in every laboratory 4,5. The alternative approach is indirect. This method involves analysing a large “healthy subpopulation”, the hypothesis being that probably more than 80% of samples stored in laboratory information systems are negative for thyroid disease and include some pre-selected criteria 6,7. Societies of laboratory medicine encourage this method in order to establish and verify TSH reference intervals 6. The TSH range obtained from a sub-population study involving “non-diseased reference individuals” can be used by endocrinologists as a threshold, below or above which therapeutic action is recommended7.
Establishing a normal reference TSH range is critical in diagnosing subclinical thyroid disorders accurately. However, there is currently no consensus regarding the optimal serum TSH level at which to initiate levothyroxine (L-T4) treatment in individuals diagnosed with subclinical hypothyroidism, particularly in the elderly 7,8. On the other hand, the evidence of the benefit of anti-thyroidal treatment in subclinical hyperthyroidism remains unclear 8, 9.
Indirect reference intervals have recently been calculated on very large populations in north-eastern Italy 10,11,12. The percentile normalization applied to TSH results obtained from 7 laboratories and 3 different immunoassays indicated similar TSH ranges in both males (0.40–4.62 mIU/l) and females (0.49–4.96 mIU/l) with a significant difference across age (e.g. lower 2.5th percentiles and higher 97.5th percentiles in subjects over 70 years of age) 11. The authors emphasised the appropriateness of defining TSH reference intervals according to age, gender and ethnicity, but did not state whether refining the TSH range according to age and sex changed the rate of diagnoses of subclinical thyroid dysfunction in comparison with the normal laboratory range 10. To our knowledge, no indirect methods have been used to define the normal TSH range in north-western Italy.
In the era of precision medicine, there seems to be a need to refine the normal range of TSH in real-world practice. The present study covers the last 20 years of TSH measurement with new-generation immunoassays in the district of Savona and neighbouring districts in Liguria and southern Piedmont (north-western Italy). A large study population of women, constituting the vast majority of subjects undergoing endocrinological investigation, was evaluated in order to determine local age-related normal TSH ranges (main outcome). A secondary objective was to reduce the overdiagnosis and over-treatment of subclinical thyroid dysfunction, which are expected to occur on a global scale.
Materials and methods
Subjects
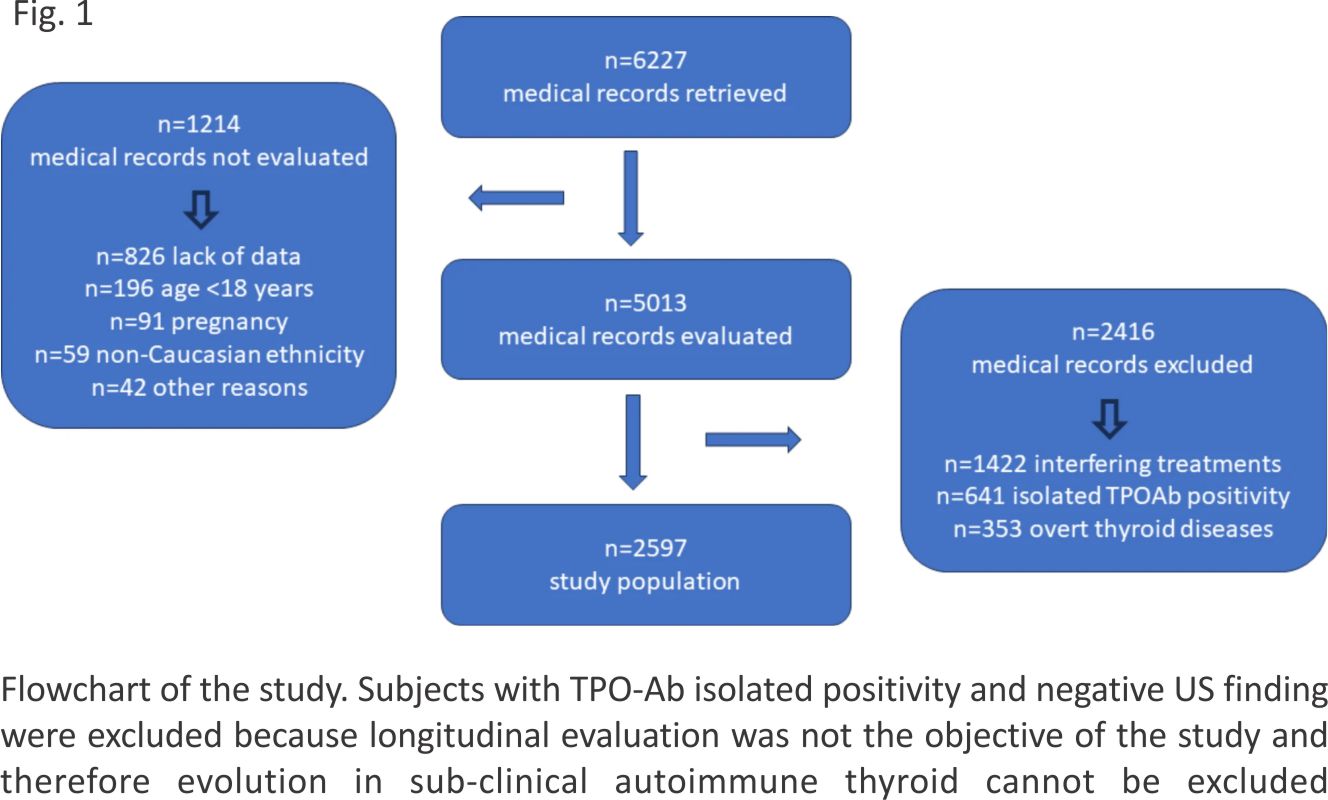
This cross-sectional, retrospective single-centre study was conducted at the Endocrine Unit of Priamar Clinical Diagnostic Centre, a private secondary-level outpatient centre located in the Savona district (Liguria, Italy). Endocrinological examination was mostly requested by general practitioners or other specialists, and sometimes directly by the patient. Examination was requested mainly for thyroid, metabolic and pituitary-gonadal or adrenal health problems, or endocrinological screening. All records collected from 2003 to 2022 were individually reviewed to ensure that the women met our inclusion criteria. We identified records of adult women who had undergone their first endocrinological examination. In this period of time, 6,227 medical records were retrieved and anonymously evaluated. Initial exclusion criteria were: lack of baseline data (incomplete records), age < 18 years, pregnancy, non-Caucasian ethnicity and other reasons. Age, body mass index (BMI), thyroid stimulating hormone (TSH), thyroid peroxidase antibodies (TPOAb), pharmacological treatments and thyroid ultrasonography (US) findings were then collected. Figure 1 shows the flow diagram of medical records of patients undergoing their first endocrinological examination from 2003 to 2022. After preliminary evaluation, 19.5% (n = 1214) of records were excluded (Fig. 1). Other reasons for exclusion were: impossibility (n = 19) or refusal (n = 8) of physical examination, male-to-female transgender (n = 6), only video consultation (n = 5), medical-legal reasons (n = 4). Subsequently, 2416 records were excluded owing to interfering treatments (58.9%; manly L-T4 administration), and TPOAb positivity with hypoechoic thyroid texture on US (26.5%) or the presence of overt thyroid diseases (14.6%; thyrotoxicosis n = 216, overt hypothyroidism n = 95, sub-acute thyroiditis n = 36, or post-partum thyroiditis n = 5). The final study sample comprised 2597 records of subjects undergoing their first endocrinological examination at the Priamar Centre (Fig. 1; for details, see Supplementary material 1). The average age of the study population at the time of the first endocrinological examination was 47.0 ± 16.9 years (± SD; range 18–90 years).
Data collection
From the medical records, the following data were anonymously transferred to Excel files: chronological age (years), district of residence, reported reason for examination, pharmacological anamnesis, smoking habits (non-smoker, previous or current smoking), body weight and height for BMI evaluation, judgement of thyroid echotexture on on-site US examination, and thyroid data (f-T4, TSH, TPOAb) close to examination. One Excel worksheet was filled in for each year from 2003 to 2022. Owing to the retrospective nature of the study, some clinical data were missing, but records were excluded from analysis only according to exclusion criteria; however, missing TPOAb data did not exclude records when thyroid US data were available. Data were retrieved from the database from June 2023 to March 2024. Data from the study population were subsequently divided arbitrarily into three age-groups: 18–44 years (n = 1200), 45–64 years (n = 934) and ≥65 years (n = 463).
Objectives
The primary objective was to obtain a local TSH range from a large group of women in whom “healthy thyroid status” had been well-defined during clinical and laboratory endocrinological examination. According to the experimental 2.5th and 97.5th percentiles of TSH, the secondary objective was to obtain the current local TSH range, whereby sub-clinical thyroid dysfunctions were diagnosed. A further objective was to compare the percentage of sub-clinical thyroid dysfunction evaluated according to TSH obtained from our study population with those from the pooled (2003–2022) TSH ranges provided by manufacturers.
Methods
Body mass index (BMI) was calculated on the basis of the weight (kg) and height (m) reported in medical files, according to the following formula: kg/m2. Smoking habits were investigated by applying a binary method (non-smoker = 0; former or current smoker = 1). All US examinations were performed by the same experienced endocrinologist (MG) using several machines (Esaote, General Electric, Fukuda Denshi), all equipped with linear probes working at 7.5–15 MHz. Data on normal thyroid volume are available for women in our district [median 8.0 ml (IQR 6.7–9.8 ml; range 3.2–19.8 ml] 13. Iodine status in the population of our districts has recently been deemed sufficient 14.
Assays
All diagnostic and laboratory tests were performed as part of routine (endocrinological) clinical care. Several commercial methods were used for f-T4 and TPOAb evaluations during the study period. Judgments of low/high f-T4 values, or negative/positive TPOAb values, were assigned according to the normal range reported by the manufacturers. In the district of Savona, two public laboratories (Santa Corona Hospital, Pietra Ligure and Azienda Sanitaria Locale 5 Savonese) and six accredited private laboratories were available for TSH assays in the study period. In this period, our centre also carried out endocrinological examinations on subjects living in the neighbouring districts of Liguria (Imperia and Genoa districts) and in an area of South Piedmont, from which Savona is easier to reach. A few TSH data came from the University of Pisa in the adjacent region of Tuscany. Overall, TSH data were obtained from 14 public and 26 private centres (for details, see Supplementary material 2). In these laboratories, the TSH range in adults is often not broken down by age or sex. Since 1999, the third-generation TSH assay has been used in all centres. All TSH calibration curves were calibrated against World Health Organisation International Reference Preparation standards (WHO IR 80/558, WHO IR 81/565).
Chemiluminescence micro-particle immunoassay (CMIA), chemiluminescent immunoassay (CLIA), electrochemiluminescence immunoassay (ECLIA), and enzyme-linked fluorescent assay (ELFA) were the automated methods used for TSH assay. Manufacturers’ TSH ranges were: CMIA: 0.35–4.5 mIU/l (ADVIA Centaur, Bayer), 0.45–5.3 mIU/l (Access TSH 3rd, Beckman Coulter Diagnostics); CLIA 0.20–3.30 miU/l (Liaison, DiaSorin), 0.30–3.74 mIU/l (Dimension VISTA, Simens), 0.35– 4.94 mIU/l (Architect System, Abbot Diagnostics), 0.40-4.0 mIU/l (Imulite, DPC), 0.46–4.68 mIU/l (Vitros, Ortho Clinical Diagnostics), 0.55–4.78 mIU/l (LOCI, Simens Healthcare Diagnostics); ECLIA 0.27–4.7 mIU/l (Elecsys Cobas, Roche Diagnostics); ELFA 0.25-5.00 mIU/l (Vidas, BioMerieux). According to the manufacturers, the functional sensitivity of the TSH assays ranged from 0.004 to 0.07 mIU/l (median: 0.01 mIU/l).
Statistical analysis
Statistical analysis was performed on a sample of 2597 medical records (study population; Fig. 1). GraphPad 10 software (GraphPad, San Diego, CA, USA) was used. Data are reported as mean ± standard deviation (SD), median, IQR, range, and 2.5th-97.5th percentiles. For statistical purposes, the functional sensitivity was set to 0.01 mIU/l, and TSH values below 0.01 mIU/l were reported as 0.01 mIU/l. Values ≤0.01 mIU/l or ≥10 mIU/l were generally excluded, as these are considered to be in the clinical hyperthyroid and hypothyroid range, respectively. The absence of normality in TSH levels was tested by means of the Kolmogorov-Smirnov test. To compare continuous data, the Kruskal-Wallis non-parametric analysis of variance was used. Percentages were compared using Fisher’s exact test. Correlations were evaluated by means of the Spearman test. Significance was set at P ≤0.05.
Ethical approval
The study was approved by the Priamar Centre’s institutional board, and a waiver of informed consent was granted because the research involved no risk to patients. Before their examination at the Priamar Clinical Diagnostic Centre, all patients had provided written informed consent to the management of data collected from their medical files and had agreed to their use for scientific purposes. Owing to the retrospective nature of the collection of clinical and hormonal data, no further formal approval from the Liguria Ethics Committee was required. Data were managed anonymously. Data collection and subsequent analysis were performed in compliance with the Helsinki Declaration.
Results
In the study period (2003–2022), TSH was evaluated by means of various commercial assays. Normality of TSH was determined according to the ranges provided by the manufacturers. Figure 2 illustrates the yearly median and range of TSH obtained by pooling the available data from the manufacturers. On non-parametric analysis of variance, no significant differences were noted among lower (P = 0.29) or upper (P = 0.78) normal TSH values from 2003 to 2022 (Fig. 2). On pooling all normal values (n = 296) available from our laboratories between 2003 and 2022, the median lower normal limit of TSH was 0.35 mIU/l (IQR 0.27–0.40 mIU/l; range 0.18–0.60 mIU/) and the median upper normal limit of TSH was 4.50 mIU/l (IQR 4.00–5.00 mIU/l range 3.00–6.00 mIU/l). The 2.5th percentile of the TSH range was 0.20 mIU/l, while the 97.5th percentile of the TSH range was 5.64 mIU/l. If f-T4 values were normal, TSH values < 0.20 mIU/l and > 5.64 mIU/l were deemed diagnostic of sub-clinical hyperthyroidism and sub-clinical hypothyroidism, respectively.
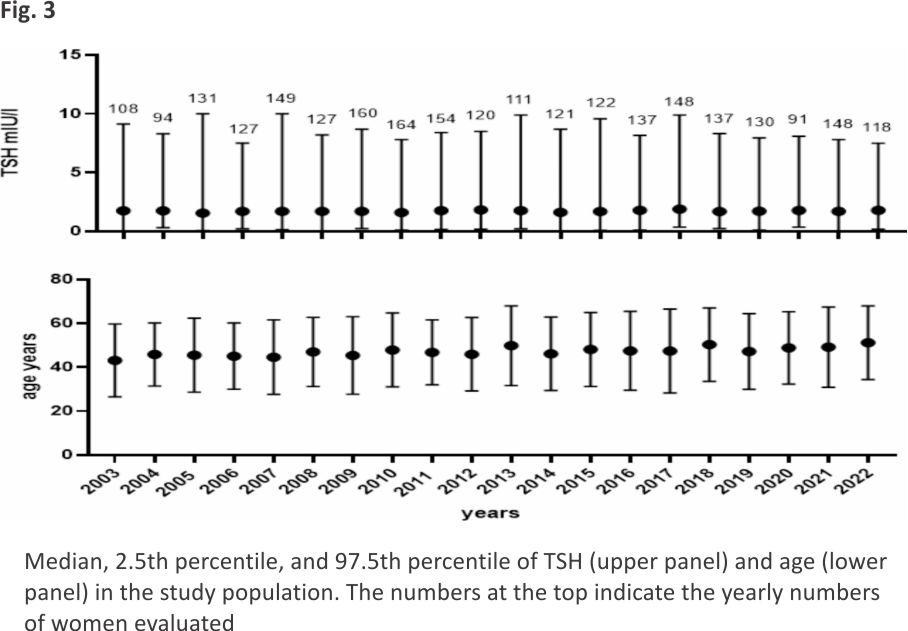
The mean age of the whole population was 47.0 years (± 16.9 years; SD; age range 18–90 years). Figure 3 shows TSH levels and age in the 2,597 records from 2003 to 2022. On analysis of variance, no significant differences among the years were observed in either TSH (P = 0.38) or age (P = 0.06) values. The yearly number of evaluable records ranged from 91 to 164 in the study period. Fewer than 100 evaluable records were retrieved in 2004, as the medical clinic in the Savona district moved its premises, and in 2020, owing to the COVID-19 pandemic. The median TSH was 1.70 mIU/l (IQR 1.20–1.75 mIU/l; range 0.02–15.62 mIU/l; 2.5th percentile 0.37 mIU/l, 97.5th percentile 6.95 mIU/l). No correlation was noted between TSH values and smoking status (n = 1552; Sr -0.02, P = 0.90) or BMI (n = 2579; Sr 0.03, P = 0.19), while a slightly significant negative correlation was found between TSH and age (n = 2579; Sr -0.04, P = 0.05).
The diagnosis and management of thyroid dysfunction focus primarily on the measurement of TSH as the most sensitive and specific marker of thyroid status 7,9. The population reference range for “normal” TSH is defined as containing 95% of a “normal” population – subjects who are believed to be free of conditions that could influence TSH levels, with 2.5% of subjects below (i.e. <2.5th percentile) and 2.5% of subjects above (i.e. >97.5th percentile) the range 1,15. Reference ranges may be device-, laboratory- and population-specific. Moreover, several other factors (gender, age, BMI, smoking, autoimmunity, and interfering substances) can influence TSH levels. Consequently, “normal” or “abnormal” TSH levels should be determined according to reference ranges from local populations and laboratories 4,8,10,11, 15,16,17,18.
In order to establish reference ranges of TSH, several studies have utilised various direct 3,17,19 and indirect 5,10,20,21 methods in normal adult populations involving from hundreds to thousands of individuals. In real-world practice, however, laboratories generally apply the TSH reference ranges suggested by assay manufacturers, without considering possible gender and age differences.
In this study, women were arbitrarily divided on the basis of the fact that middle age is generally defined as the time from about 40–45 years to about 60 − 35 years, and the elderly are defined as persons aged 65 years and older. We determined age-related TSH in a cohort of women whose clinical characteristics, hormonal data, US findings and therapies were known. All the women in our study population (n = 2,597) were adults (≥18 years) and Caucasian. About 70% were living in the Savona district. In the period 2003–2022, the median female (≥20 years) population of the Savona district was 126,500 individuals 22. We therefore estimated that our study population involved about 1% of adult women living in the Savona district. Our median TSH was 1.70 mIU/l, with a percentile interval ranging from 0.37 mIU/l (2.5th percentile) to 6.95 mIU/l (97.5th percentile). These data are not strictly comparable with those obtained using a direct procedure in the Pordenone district (Friuli; north-eastern Italy) in “normal” volunteer women aged 20–65 years (i.e. no detectable autoantibodies, no history of thyroid dysfunction, non-palpable goiter, no interfering drugs), in whom the median TSH and 2.5th percentile were 1.66 mIU/l and 0.56 mIU/l, but the 97.5th percentile was set to 3.27 mIU/l 10. This difference could be explained by the different upper age ranges in the study by Tozzoli et al. 10 (up to 65 years) and ours (≥65 years). On the other hand, in a sample of 8619 girls (> 12 years of age) and women without a history of thyroid disease, in the USA, the median TSH level was 1.50 mIU/l and the 97.5th percentile was 6.10 mIU/l 23. In Sicily, a TSH reference range was determined by applying indirect methods to a large dataset (n = 22,602) stored in a laboratory from 2012 to 2018. Only a minority of data had been obtained from outpatients (12%), and information on possible interfering therapies, BMI, smoking status and thyroid morphology was lacking 4. In women, the lower limit of the reference range (0.18 mIU/l) was similar to that provided by manufacturers (0.20 mIU/l), but the upper limit was calculated as 3.94 mIU/l, as opposed to the manufacturers’ limit of 4.70 mIU/l 4. In that study, median TSH values decreased with age, as noted in our population, with a slight negative correlation between age and TSH.
In one of our previous studies, a borderline status of iodine sufficiency (101 µg/l) was noted in a cohort of adult subjects living in our district 14, and it may be supposed that the iodine status of the present study population was similar. Moreover, it has been reported that TSH may be higher in areas of both overt and partial iodine deficiency24. Indeed, in a study conducted in areas with excessive iodine intake, the 97.5th percentile of TSH in adult females (all ages) was set to 8.42 mIU/l 25. While past or current smoking has been associated with lower TSH levels 26, the effect of smoking in our population of women can be considered marginal or absent. Regarding the relationship between BMI and TSH, there is no consensus in the literature, and both positive 27,28 and negative 29 correlations have been reported. In agreement with our data on women, Ivo et al. 28 found no significant correlation between BMI and TSH, even when a reference population of euthyroid subjects (normal TSH) was separately evaluated according to sex.
In our study, the 97.5th percentile of TSH increased by about 1.00 mIU/l per age group, rising from 5.94 mIU/l to 7.69 mIU/l, while in other studies, 4,10 it remained stable throughout life. Moreover, it is well known that the distribution curve of normal TSH is shifted to the right in the elderly, 30, and several other studies have shown an increasing trend in the 97.5th percentile of TSH with age. In the Padoan et al. 12 study, women referred for TSH evaluation by general practitioners showed a slightly increasing TSH trend (from 4.96 mIU/l to 5.48 mIU/l) on passing from the ≤35-year group to the ≥70-year group. Other studies have reported an age-related increase in TSH, with the 97.5th percentile exceeding 7.0 mIU/l in individuals aged over 80 years 23,30,31. Similar findings emerged from older data in Tuscany (Central Italy), with TSH measured by means of radio-immunoassay; in a small group of very elderly subjects (≥100 years), however, median TSH levels were lower than in subjects aged 20–64 years 32. In a recent study by Luxia et al. 33, in which Han subjects with normal thyroid function were stratified into three age-groups (young: 18–44 years, middle-aged: 45–59 years, and elderly: >60 years), females, but not males, displayed a similar gradual increase in TSH, which peaked in middle age and subsequently declined.
Taylor et al. 30 reported an increase in hypothyroidism in the UK between 2005 and 2014 in subjects aged over 60 years, with a consequent increase in L-T4 initiation. On the other hand, in a recent investigation of the incidence and determinants of spontaneous TSH normalisation in subjects > 65 years old with an initial TSH value between 4.60 and 19.99 mIU/l, van der Spoel et al. 34 observed that the hormone had spontaneously normalised after about 1 year in about 61% of subjects. After a further year, the same phenomenon was observed in 40% of subjects with abnormal TSH, randomised to placebo 34. Interestingly, female sex, negative TPOAb, less elevated TSH, higher initial f-T4 and TSH measurement in summer were independent determinants of normalisation. The practical implication of this is that it may be advisable to wait at least one year before starting L-T4 treatment when TSH levels are above the manufacturer’s range but below the population-derived age-related 97.5th percentile. Our study, therefore, suggests that, in the district of Savona and nearby areas, women with TSH levels above this percentile could be treated for sub-clinical hypothyroidism. However, according to the literature 34, the risk of unnecessary L-T4 treatment might require a longitudinal evaluation of TSH. In addition, we observed that, on redefining the upper limit of normal TSH, the incidence of sub-clinical hypo- thyroidism significantly decreased in subjects over 45 years of age when “study population” TSH ranges were adopted rather than laboratory-derived TSH ranges years, as observed in subjects > 65 years of age in other studies 8,35, an approach that prevents over-treatment.
Nevertheless, inappropriate anti-thyroidal treatment could be started in a supposed condition of sub-clinical hyperthyroidism when f-T4 is in the normal range but TSH is lower than the manufacturer’s reference range. The decision to undertake a pharmacological approach must always be carefully considered, particularly in the elderly, in whom it is well known to engender a higher risk of all-cause mortality and cardiovascular morbidity and mortality 9. Indeed, in a recent meta-analysis involving 134,346 participants with a median age of 59 years (range 18–106 years), f-T4 greater than the 85th percentile and TSH below the 20th percentile, 4.3% of whom were on thyroid medication at baseline, the authors reported a higher risk of all-cause mortality and cardiovascular mortality 36.
In our study, the TSH value set at the 2.5th percentile was slightly lower in the 18-44-year age group (0.49 mIU/l) than in the other two age groups (0.30 mIU/l). A similar pattern has been reported in some 4,12,31,37, but not all, studies 8,38. Differences among studies could stem from inhomogeneous division into subgroups, different sample sizes, iodine status and other reasons, including the assignment of subjects with pre-clinical thyroid nodular hyperfunction to the category of “normal” elderly women. From our data, the suspicion of sub-clinical hyper-function seems slightly more frequent on applying the “study range” instead of the “manufacturer” range, especially in the group of women aged 18–44 years. This observation suggests that the lower limit of the reference TSH range may also need to be reassessed, as reported by Xu et al. 36.
The present study has several limitations. Firstly, the reference limits of laboratories vary greatly (see supplemental materials) and lumping these data together could hamper our findings; however, an ideal mixed model or stratification by assay was not possible. Secondly, age-related changes in the TSH range were not compared between females and males. In our experience, however, the demand for endocrinological examination in young and middle-aged males is quite low. Nevertheless, we hope to perform a similar cross-sectional study of a large dataset on males soon. Thirdly, our group of “normal healthy” women aged ≥65 years was smaller than the other two age-groups. However, our study population was larger than the minimum recommended limit in direct studies aimed at determining a normal range 3. Moreover, a selection bias could have emerged from our cross-sectional study of subjects undergoing their first endocrinological investigation for several reasons, though strict exclusion criteria were applied. Indeed, it seems easier to identify a population free from clinical thyroid problems in data from national studies 4,10,12 employing “big data”. In addition, on-site ultrasonography screening was routinely added, as in other studies 18,25,38. Finally, the women who underwent endocrinological examination at our centre might not be representative of the general population of our districts, owing to the expense of attending a private centre. However, the average income in our districts is not so low as to make socioeconomic status a real problem, and our study group represented about 1% of women living in the Savona district. Moreover, in the period 2003–2022, no age-related TSH range was available at public healthcare centres in Liguria. A further limitation of our study could be the incompleteness of data on thyroid hormones in the first endocrinological examination.
Serum TSH reference ranges differ across laboratories 8,39. By Razvi et al. 39, we sought to determine, in healthy women, a TSH range based more on clinical outcomes than on statistical techniques.
In conclusion, this is the first study in Liguria to establish new age- and gender-specific reference values for TSH. Based on a large number of women, this new age-related range could be more extensively employed to improve diagnoses. The main result of implementing age- and gender-related normal TSH levels between the 2.5th and 97.5th percentiles seems to be a slight increase in the number of 18-44-year-old women with sub-clinical hyperthyroidism and a very significant reduction in the hasty diagnosis of sub-clinical thyroid dysfunction in women aged 45–64 years and ≥65 years. Therapies for thyroid dysfunction must be started when TSH is outside age-related ranges, according to the patient’s clinical condition and when this finding is confirmed some time later.
Data availability
No datasets were generated or analysed during the current study.
References
1. Razvi S. Thyroid-function reference ranges in the diagnosis of thyroid dysfunction in adults. Nat Rev Endocrinol. 2024;20(5):253–4. https://doi.org/10.1038/s41574-024-00972-2.
2. Spencer CA. Laboratory thyroid tests: a historical perspective. Thyroid. 2023;33(4):407–19. https://doi.org/10.1089/thy.2022.0397.
3. Clinical and Laboratory Standards Institute (CLSI). Defining, establishing, and verifying reference intervals in the clinical laboratory; approved guidelines. CLSI Socument EP28-A3c. 3rd ed.;28:pp1–59.Wayne PA.
4. Lo Sasso B, Vidali M, Scazzone C, Agnello L, Ciaccio M. Reference interval by the indirect approach of serum thyrotropin (TSH) in a Mediterranean adult population and the association with age and gender. Clin Chem Lab Med.2019; 57(10):1587–94. https://doi.org/ 10.1515/cclm-2018-0957.
5. Grossi E, Colombo R, Cavuto S, Franzini C. The REALAB project: a new method for the formulation of reference intervals based on current data. Clin Chem. 2005; 51(7):1232–40. https://doi.org/ 10.1373/clinchem.2005.047787
6. Katayev A, Balciza C, Seccombe DW. Establishing reference intervals for clinical laboratory test results: is there a better way? Am J Clin Pathol. 2010;133(2):180–6. https:// doi.org/10.1309/AJCPN5BMTSF1CDYP.
7. Biondi B, Cappola AR. Subclinical hypothyroidism in older individuals. Lancet Diabetes Endocrinol. 2022; 10(2):129–41. https://doi.org/10. 1016/S2213-8587(21)00285-0.
8. Yamada S, Horiguchi K, Akuzawa M, Sakamaki K, Yamada E, Ozawa A, et al. The impact of age- and sex-specific reference ranges for serum thyrotropin and free thyroxine on the diagnosis of subclinical thyroid dysfunction: a multicenter study from Japan. Thyroid. 2023;33(4):428–39. https://doi.org/10.1089/thy.2022.0567.
9. Biondi B, Cooper DS, Subclinical Hyperthyroidism. N Engl J Med. 2018;378(25):2411–9. https:// doi.org/10.1056/NEJMcp1709318.
10. Tozzoli R, D’Aurizio F, Metus P, Steffan A, Mazzon C, Bagnasco M. Reference intervals for thyrotropin in an area of Northern Italy: the Pordenone thyroid study (TRIPP). J Endocrinol Invest. 2018;41 (8):985–94. https://doi.org/10. 1007/s40618-018-0825-0.
11. Clerico A, Trenti T, Aloe R, Dittadi R, Rizzardi S, Migliardi M, et al. Italian section of the European Ligand Assay Society (ELAS). A multicenter study for the evaluation of the reference interval for TSH in Italy (ELAS TSH Italian Study). Clin Chem Lab Med. 2018;57(2):259–67. https://doi.org/10.1515/cclm-2018-0541.
12. Padoan A, Clerico A, Zaninotto M, Trenti T, Tozzoli R, Aloe R, et al. Percentile transformation and recalibration functions allow harmonisation of thyroid-stimulating hormone (TSH) immunoassay results. Clin Chem Lab Med. 2020; 58(10):1663–72. https://doi.org/ 10.1515/cclm-2019-1167.
13. Giusti M, Sidoti M. Normal thyroid volume in subjects evaluated in a primary ambulatory setting in Liguria. Minerva Endocrinol (Torino). 2023;48(1):19–26. https://doi. org/10.23736/S2724-6507.20. 03312-X.
14. Conte L, Comina M, Monti E, Sidoti M, Vannozzi O, Di Ciolo L, et al. Urinary iodine concentration in a cohort of adult outpatients with thyroid diseases in Liguria, 14 years after the law on salt iodisation. Nutrients. 2019;12(1):11. https: //doi.org/10.3390/nu12010011.
15. Razvi S, Bhana S, Mrabeti S. Challenges in interpreting thyroid-stimulating hormone results in the diagnosis of thyroid dysfunction. J Thyroid Res. 2019;2019:4106 816. https://doi.org/10.1155/ 2019/4106816.
16. Vadiveloo T, Donnan PT, Murphy MJ, Leese GP. Age- and gender-specific TSH reference intervals in people with no obvious thyroid disease in Tayside, Scotland: the thyroid epidemiology, audit, and Research Study (TEARS). J Clin Endocrinol Metab. 2013;98(3): 1147–53. https://doi.org/10. 1210/jc.2012-3191.
17. Cai J, Fang Y, Jing D, Xu S, Ming J, Gao B, et al. Reference intervals of thyroid hormones in a previously iodine-deficient but presently more than adequate area of Western China: a population-based survey. Endocr J. 2016;63(4):381–8. https://doi.org/10.1507/endocr
18. Gurgel MHC, Ponte CMM, Fontes R, Rocha ÍV, Batista LAA, Sousa TCS, et al. Establishment of reference interval for thyroid-stimulating hormone using electrochemiluminescence assay in a healthy adult population from Fortaleza, Brazil. Arch Endocrinol Metab. 2020;64(4):362–8. https://doi.org/10.20945/2359-3997000000264.
19. Hamilton TE, Davis S, Onstad L, Kopecky KJ. Thyrotropin levels in a population with no clinical, autoantibody, or ultrasonographic evidence of thyroid disease: implications for the diagnosis of subclinical hypothyroidism. J Clin Endocrinol Metab.2008;93(4): 1224–30. https://doi.org/10. 1210/jc.2006-2300.
20. Jones GRD, Haeckel R, Loh TP, Sikaris K, Streichert T, Katayev A, et al. IFCC Committee on Reference Intervals and decision limits. Indirect methods for reference interval determination – review and recommendations. Clin Chem Lab Med. 2018;57(1):20–9. https://doi. org/10.1515/cclm-2018-0073.
21. Giavarina D, Dorizzi RM, Soffiati G. Indirect methods for reference intervals based on current data. Clin Chem. 2006;52(2):335–7. https://doi.org/10.1373/clinchem.2005.062182.
22. Tuttitalia.itStatistiche.demogra- fiche provincia di Savona 2002– 2022. https://www.tuttitalia.it/ liguria/provincia-di-savona/ statistiche/popolazione
23. Hollowell JG, Staehling NW, Flanders WD, Hannon WH, Gunter EW, Spencer CA, et al. Serum TSH, T(4), and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab. 2002; 87 (2):489–99. https://doi.org/10. 1210/jcem. 87.2.8182.
24. Zimmermann MB, Boelaert K. Iodine deficiency and thyroid disorders. Lancet Diabetes Endocrinol. 2015; 3(4):286–95. https://doi.org/10. 1016/S2213-8587(14)70225-6.
25. Kim M, Kim TY, Kim SH, Lee Y, Park SY, Kim HD, et al. Reference interval for thyrotropin in an ultrasonography-screened Korean population. Korean J Intern Med. 2015;30(3):335–44. https://doi.org/10.3904/kjim.2015.30.3.335.
26. Asvold BO, Bjøro T, Nilsen TI, Vatten LJ. Tobacco smoking and thyroid function: a population-based study. Arch Intern Med. 2007; 167(13):1428–32. https://doi.org /10.1001/archinte.167.13.1428.
27. Abdi H, Faam B, Gharibzadeh S, Mehran L, Tohidi M, Azizi F, et al. Determination of age and sex specific TSH and FT4 reference limits in overweight and obese individuals in an iodine-replete region: Tehran thyroid study (TTS). Endocr Res. 2021;46(1): 37–43. https://doi.org/10. 1080/07435800.2020.1854778.
28. Mele C, Mai S, Cena T, Pagano L, Scacchi M, Biondi B, et al. The pattern of TSH and fT4 levels across different BMI ranges in a large cohort of euthyroid patients with obesity. Front Endocrinol (Lausanne). 2022;13:1029376. https://doi.org/10.3389/fendo.2022.1029376.
29. Ivo CR, Duarte V, Veríssimo D, Silva J, Passos D, Lopes L, et al. Thyrotropin and body mass index, are they related? Horm Mol Biol Clin Investig. 2022;44(1):1–4. https://doi.org/ 10.1515/hmbci-2022-0002.
30. Taylor PN, Lansdown A, Witczak J, Khan R, Rees A, Dayan CM, et al. Age-related variation in thyroid function – a narrative review highlighting important implications for research and clinical practice. Thyroid Res. 2023;16(1):7. https:// doi.org/10.1186/s13044-023-00149-5.
31. Surks MI, Boucai L. Age- and race-based serum thyrotropin reference limits. J Clin Endocrinol Metab. 2010;95(2):496–502. https://doi.org/10.1210/jc.2009-1845.
32. Mariotti S, Barbesino G, Caturegli P, Bartalena L, Sansoni P, Fagnoni F, et al. A. Complex alteration of thyroid function in healthy centenarians. J Clin Endocrinol Metab. 1993;77(5):1130–4. https://doi.org/10.1210/jcem.77.5.8077303.
33. Luxia L, Jingfang L, Songbo F, Xulei T, Lihua M, Weiming S, et al. Correlation between serum TSH levels within the normal range and serum lipid profile. Horm Metab Res. 2021;53(1):32–40. https://doi.org/10.1055/a-1191-7953.
34. van der Spoel E, van Vliet NA, Poortvliet RKE, Du Puy RS, den Elzen WPJ, Quinn TJ, et al. Incidence and determinants of spontaneous normalisation of subclinical hypothyroidism in older adults. J Clin Endocrinol Metab. 2024;109(3):e1167–74. https://doi.org/10.1210/clinem/dgad623.
35. Yildiz Z, Dağdelen LK. Reference intervals for thyroid disorders calculated by the indirect method and comparison with reference change values. Biochem Med (Zagreb). 2023;33(1):010704. https://doi.org/10.11613/BM.2023.010704.
36. Xu Y, Derakhshan A, Hysaj O, Wildisen L, Ittermann T, Pingitore A, Thyroid Studies Collaboration, et al. The optimal healthy ranges of thyroid function defined by the risk of cardiovascular disease and mortality: systematic review and individual participant data meta-analysis. Lancet Diabetes Endocrinol. 2023;11(10):743–54. https://doi. org/10.1016/S2213-8587(23) 00227-9.
37. Adams R, Oh ES, Yasar S, Lyketsos CG, Mammen JS. Endogenous and exogenous thyrotoxicosis and risk of incident cognitive disorders in older adults. JAMA Intern Med. 2023;183(12):1324–31. https:// doi.org/10.1001/jamainternmed.2023.5619.
38. Lu Y, Zhang WX, Li DH, Wei LH, Zhang YJ, Shi FN, et al. Thyroid hormone reference intervals among healthy individuals in Lanzhou, China. Endocrinol Metab (Seoul). 2023;38(3):347–56. https://doi.org/10.3803/EnM.2023.1638.
39. Razvi S, Jabbar A, Addison C, Vernazza J, Syed A, Soran H, et al. Variation in the reference range limits of thyroid function tests and association with the prevalence of levothyroxine treatment. Eur J Endocrinol. 2023;188(2):lvad016. https://doi.org/10.1093/ejendo/lvad016.
Acknowledgements
We thank Bernard Patrick for revising the language of the paper.
Funding
No funding was received.
Author information
Authors and Affiliations
Endocrine Unit, Centro Clinico Diagnostico Priamar, Via dei Partigiani 13R, Savona, 17100, Italy
Massimo Giusti & Marilena Sidoti
Dipartimento di Medicina Interna, Università di Genova, Genoa, Italy
Massimo Giusti
Endocrine Unit, Azienda Sanitaria Locale 2 Savonese, Savona, Italy
Marilena Sidoti
Contributions
M.G. and M.S. carried out this research. M.G. and M.S. were responsible for data collection. M.G. wrote the manuscript text. All authors reviewed and approved the final version of the manuscript.
Corresponding author
Correspondence to Massimo Giusti.
Ethics declarations
Ethical approval and consent to participate
All procedures were carried out under the ethical standards of the institution and with the 1975 Helsinki Declaration, as revised in 2008. Informed consent was obtained from all women.
Author Disclosure Statement
No competing financial interests exist.
Competing interests
The authors declare no competing interests.
Credit: Giusti, M., Sidoti, M. Women-specific reference ranges for serum TSH in Liguria: the impact of age and year of collection in a single-centre cross-sectional study. Thyroid Res 18, 8 (2025). https:// doi.org/10.1186/s13044-025-00225-y