

Robert B. Barrett, Benjamin Riesser, Benjamin Martin, Neha Sachdev, Michael K. Rakotz, Susan E. Sutherland, and Brent M. Egan
Abstract
BACKGROUND:
Adults with hypertension have fewer cardiovascular events if controlled within the first 6 months of diagnosis, during which time they are excluded from many hypertension control metrics. We compared blood pressure (BP, mm Hg) control rates from 6 to 42 months in adults with hypertension who did or did not have anti-hypertensive treatment initiated (TI) with monotherapy during the first month after diagnosis, irrespective of subsequent changes in antihypertensive pharmacotherapy.
METHODS:
A retrospective cohort of 15,422 patients, mean age 56.0±14.8 years, from 5 health care organizations, was identified with previously undiagnosed and untreated hypertension. BP control (<140/<90) and TI on visits with uncontrolled readings were assessed as a function of time since diagnosis, up to 42 months. Logistic regression models provided estimates of the odds of TI for initial BP, stratified by race, sex, and diagnosed diabetes. Cox proportional hazards regression estimated the hazard ratio of BP control over time.
RESULTS:
Patients with TI during the first month versus later time points had better BP control at 6 (57.7% versus 47.7%, P<0.001) through 30 months (66.8% versus 62.2%, P<0.001), with similar control rates thereafter.
CONCLUSIONS:
TI within the first month after diagnosis in contrast to later time points, leads to better BP control at 6 to 30 months, which is associated with better clinical outcomes and performance on standard hypertension control metrics. While better control is sustained for 30 months, treatment with monotherapy during the first month following diagnosis was insufficient to control hypertension in >30% of patients.
NOVELTY AND RELEVANCE
What Is New?
In adults with untreated and uncontrolled hypertension, starting monotherapy within the first month after diagnosis versus later time points provides better blood pressure control from 6 to 30 months after diagnosis.
What Is Relevant?
Despite better blood pressure control with prompt treatment initiation, many remain uncontrolled, suggesting that subsequent treatment intensification is insufficient.
Confirming uncontrolled hypertension through repeated measurement during a medical encounter increases the probability of treatment initiation.
Clinical/Pathophysiological Implications?
Prompt initiation of antihypertensive therapy and timely intensification at subsequent visits are keys to better blood pressure control.
The benefits of antihypertensive pharmacotherapy accrue rapidly in primary care and clinical trials. When better blood pressure (BP, mm Hg) control is achieved during the first 3 to 6 months of treatment, fewer cardiovascular events occur during this time interval. 1–5 Standard hypertension control metrics typically exclude patients during the first 6 months following diagnosis, after which time they are included.6 Thus, for both clinical outcomes and care quality metrics, controlling hypertension within the first 6 months after diagnosis is important.
Prompt initiation of antihypertensive pharmacotherapy is a key to realizing the time-sensitive benefits of BP reduction. Antihypertensive monotherapy is the norm for treatment initiation in clinical practice, despite evidence that monotherapy is insufficient to control hypertension in most patients. Furthermore, the 2017 American College of Cardiology/American Heart Association high BP guideline recommends treatment initiation with 2 different antihypertensive medications when BP is ≥20/≥10 mm Hg above the target.7 Previous research indicates that not only are most adults with hypertension initiated on antihypertensive monotherapy, but also that most of them remain on monotherapy at 3 years.8 Moreover, half of the adults with uncontrolled hypertension were on monotherapy after 8 years.9
Given the evidence, our study was designed to determine if initiating treatment with antihypertensive monotherapy (TI) during the first month after the diagnosis of hypertension that was uncontrolled led to more prompt and better BP control over time than when TI did not occur in the first month. A secondary objective was to identify factors associated with the decision to initiate treatment during the first month following diagnosis of hypertension than later time points.
METHODS
Regulatory Considerations
This secondary analysis of a limited data set from the American Medical Association (AMA) Measure Accurately, Act Rapidly, Partner with Patients (MAP) Hypertension quality improve- ment program was reviewed by the institutional review board at the University of Illinois (Federal Wide Assurance 00000083), the institutional review board of record for the AMA, and determined not to meet the definition of human subjects research. The Strengthening the Reporting of Observational Studies in Epidemiology guidelines were used.10 The Business Associate Agreements between the AMA and participating health care systems do not permit data sharing. The authors provided all critical data in the article.
The MAP Hypertension quality improvement program has been described.11 Briefly stated, the program focuses on 4 key process measures for improving hypertensive population BP (mm Hg) control rates: measure accurately, assessed by documenting a confirmatory (repeat) measurement following an uncontrolled BP reading (systolic BP [SBP] ≥140 or diastolic BP [DBP] ≥90); Act rapidly, defined as therapeutic intensification for uncontrolled hypertension; and 2 partner with patients metrics defined as: (1) the percentage of patients having a ≥10 mm Hg reduction in SBP within 7 to 180 days after adding a new antihypertensive medication class, and (2) a follow-up BP measurement within 30 days of an outpatient visit where BP was uncontrolled. This study focused on the effects of TI within the first 30 days after diagnosis, compared with later periods, on hypertension control.
Data Source
Patient data were obtained from the electronic medical record systems of 5 participating health care organizations or data warehouses containing electronic medical record data. These organizations located in the Southeast and Midwest, included 2 federally qualified health centers, a private, a county, and a university hospital-based health system. The data were then cleaned (eg, SBPs >300 or <80 were excluded), normalized for unit of measure (eg, height, weight), and then ingested into a relational database using a custom common data model for harmonization between disparate systems. Analytical datasets were created in the form of limited data sets by removing individually identifiable data elements, both through masking and element exclusion. Dates of service were retained.
Inclusion Criteria
Patients were required to have a visit between January 2019 and January 2023 where essential hypertension (International Classification of Disease, Tenth Revision, Clinical Modification code I10) was first recorded in the electronic medical record and SBP ≥140 or DBP ≥90, and at least 1 visit at a participating program site before and after the diagnosis of hypertension. The requirement of at least 1 prior visit before receiving the diagnosis of hypertension was intended to increase the likelihood that the cohort was comprised of newly diagnosed patients. Follow-up visits for up to 42 months after the initial diagnosis were included.
Exclusion Criteria
Patients <18 or >85 years were excluded, which is consistent with the age range used in other quality metrics for controlling BP.6 Patients with prescriptions for antihypertensive medications before the initial diagnosis of hypertension were also excluded.
Body mass index (kg/m2) was calculated from height, measured intermittently, and weight, which was recorded on 85% of encounters.
BP values were obtained from primary care practice sites of participating institutions. If >1 BP value was recorded for an encounter, the minimum SBP and corresponding DBP were selected for analysis.
Hypertension was defined by an International Classification of Diseases, Tenth Revision, Clinical Modification diagnostic code of I10. For this study, only patients with newly diagnosed and untreated hypertension were included. Un-treated hypertension was defined as individuals with an initial visit BP of 140/90 mm Hg or greater without previously prescribed antihypertensive medication.
Time since diagnosis was calculated as the number of months from the visit date of the first observed hypertension diagnosis.
Hypertension control was defined by a medical encounter with SBP <140 and DBP <90. Visits were grouped into periods of 6 months, with BP control calculated as the percentage of encounters with BP <140/<90 for each patient.
TI was defined by a new prescription for an antihypertensive medication class in previously untreated patients with uncontrolled BP.
Treatment intensification, which includes TI, was defined as a new prescription for an antihypertensive medication class in a patient with uncontrolled hypertension, irrespective of whether the patient was treated or untreated.
An outpatient encounter was defined by data indicating that a patient received service from a clinician at a primary care program site, either in-person or virtually. Inpatient visits, cancelled appointments, and visits where the context was indicated as emergency, documentation only, or another nonclinical encounter were not included in the analytic data set.
Monotherapy was defined as treatment initiation with an anti-hypertensive medication of a single drug class.
Combination therapy was defined as coincident treatment with >2 antihypertensive medication classes.
Diabetes was identified from the International Classification of Diseases, Tenth Revision coding in the electronic health record system.
Data analysis was conducted using a combination of Structured Query Language (SQL) and Python libraries, including StatsModels (0.13.2), Lifelines (0.28.0), NumPy (1.21.5), and Pandas (1.4.4). Clinical and demographic characteristics of the patient cohort were summarised as the number and frequency for categorical data or mean and standard deviation (SD) for continuous data. Comparisons of characteristics for patients with TI during the first month following diagnosis versus those without treatment in the first month were conducted using χ2 statistics or pooled t tests. Patient characteristics were also examined at 3 time points, including 1 month, 24 months, and 42 months, to assess potential bias in loss to follow-up in the analysis cohort.
The primary analysis considered 2 outcomes of interest: (1) the incidence of TI during the first month since diagnosis versus later time points, and (2) BP control to <140/ <90. Both outcomes were calculated as prevalence ratios for visits within 6-month intervals, with the first month following the diagnosis serving as the initial value. Multi-variable models incorporated age, race, sex, diabetes, initial BP, and a confirmatory or repeat BP after an initial SBP ≥140 or DBP ≥90 as independent variables. Race was dichotomised as White or non-White by combining Black and other than White races. The relationship between each dependent variable and independent variable was examined as a function of time since diagnosis, comparing patients initiated on monotherapy to those remaining untreated during the first month following initial diagnosis of hypertension. Variables for each model were predetermined, and potential effect modification was assessed by the inclusion of interaction terms in the model. When no significant effect modifications were detected, the interaction terms were omitted from the final model. Potential confounding effects were examined using stratified models to assess their influence.
Logistic regression models were used to compute the odds of TI for each 10 mm Hg increase in SBP and DBP, the presence of confirmatory BP measurements, and for each 5-year increment in patient age. Logistic regression models were constructed for the cohort and separately for patients with and without diabetes, for White and non-White race, and by sex. Models were not adjusted for body mass index, as this variable did not affect model outcomes. Cox proportional hazards regression was performed to estimate the rate of BP control over the 42-month study period (at both <140/<90 and <130/<80) for patients with TI in the first month compared with patients without TI in the first month. For all multivariable models, observations were limited to covariates with non-missing data.
RESULTS
A patient cohort was selected from 5 health care organisations participating in the AMA MAP Hypertension quality improvement program to improve BP control (Figure 1). In this study, 15,422 eligible patients with 63,558 clinical encounters were followed for up to 42 months. Of these clinical encounters, 313 (0.5%) were without a documented race, and 10,850 (15%) without a body mass index. The median length of follow-up was 24 months overall, 18 months for patients with TI during the first month, and 24 months for those without TI in the first month.
Table 1 shows the demographic and clinical characteristics for all patients during the first month following hypertension diagnosis and stratified by treatment status in the first month. Non-White, female, younger ages, and those with higher BP values were more likely to have TI in the first month. Patients diagnosed with diabetes were less likely to have TI in the first month.
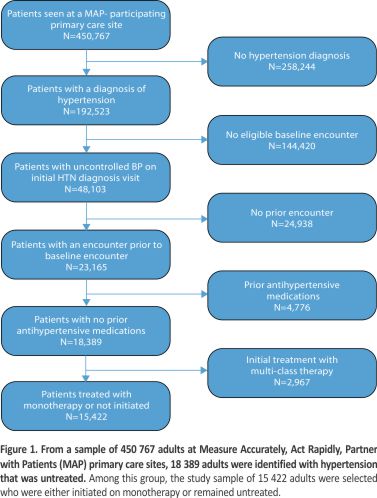
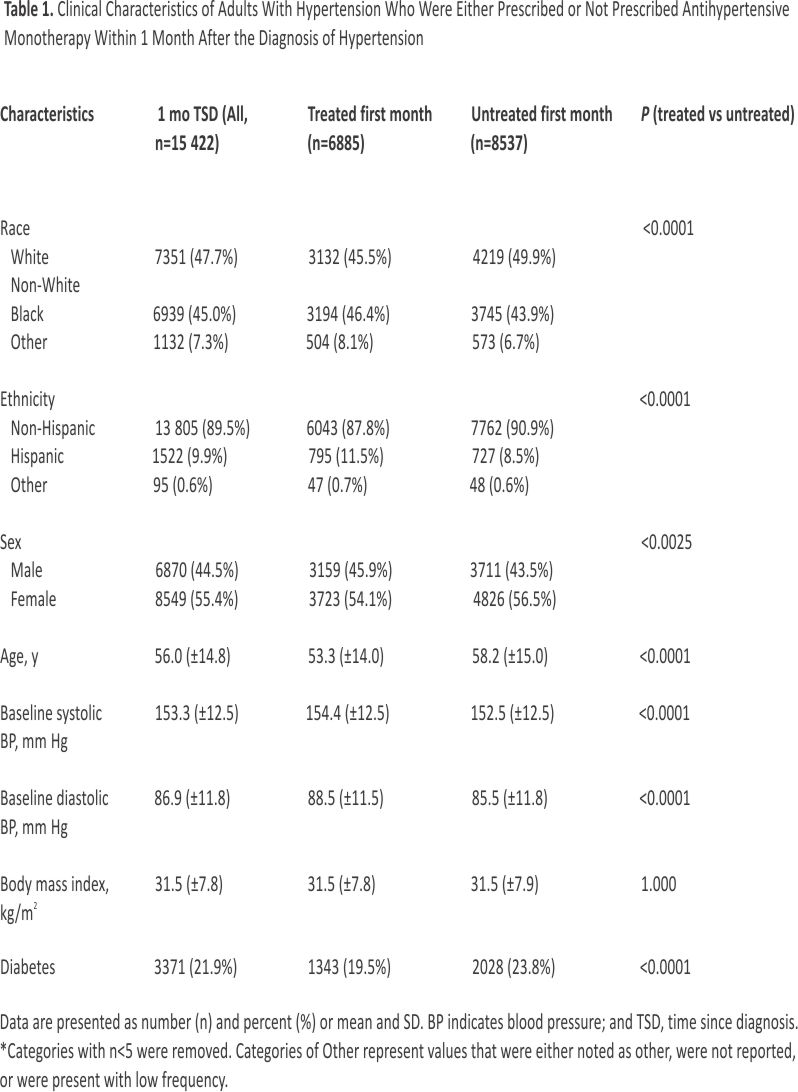
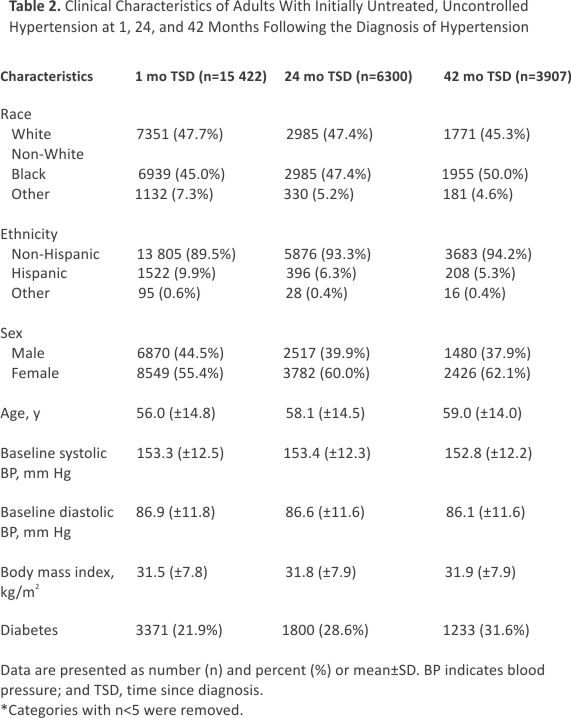
Table 2 captures demographic and clinical characteristics over the follow-up period. Those with longer follow-up time were more likely to be female, older and have diabetes. Initial SBP and DBP values were similar across time points.
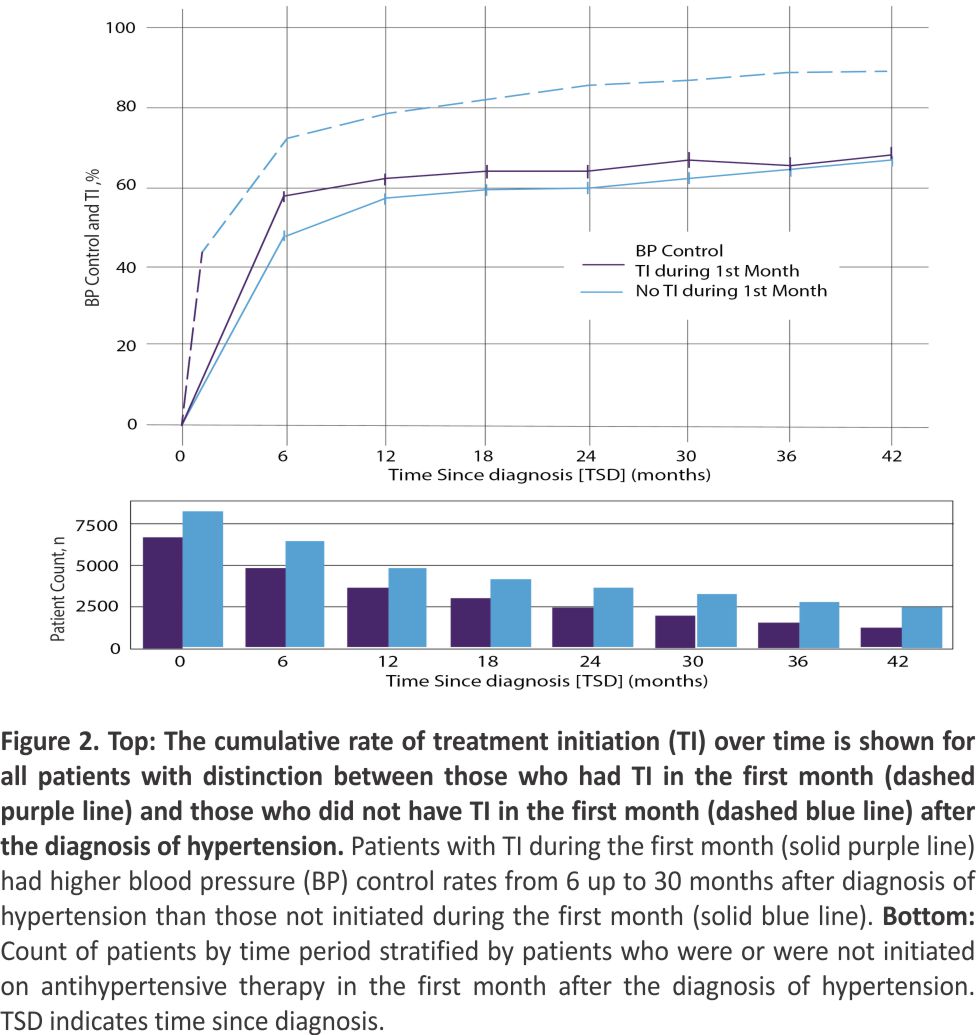
TI with monotherapy for uncontrolled hypertension was evaluated during the first month after diagnosis and at 6-month intervals thereafter (Figure 2). TI occurred in ≈44% of patients in the first month, 75% at 6 months, 82% at 1 year, and 90% at 2 years after diagnosis. The influence of TI with monotherapy during the first month after the diagnosis of hypertension versus later time points on BP control to <140/<90 at 6-month intervals is also shown in Figure 2. Patients with TI during the first month had a significantly higher control rate at 6 months since diagnosis (57.4% versus 47.5%, P<0.001), which was maintained until 30 months (66.8% versus 62.0%, P<0.001). Further, patients treated in the first month had only a 1.9 mm Hg greater baseline mean SBP than their untreated counterparts, although the difference was statistically significant (154.4 versus 152.5 mm Hg, P<0.001).
The rate of treatment intensification for those who did and did not begin monotherapy in the first month is shown in Figure S1. For patients with TI during the first month, values from 6 through 42 months represent the rate of subsequent treatment intensification. For those who were not initiated on monotherapy in the first month, values from 6 through 42 months represent both TI and subsequent treatment intensification.
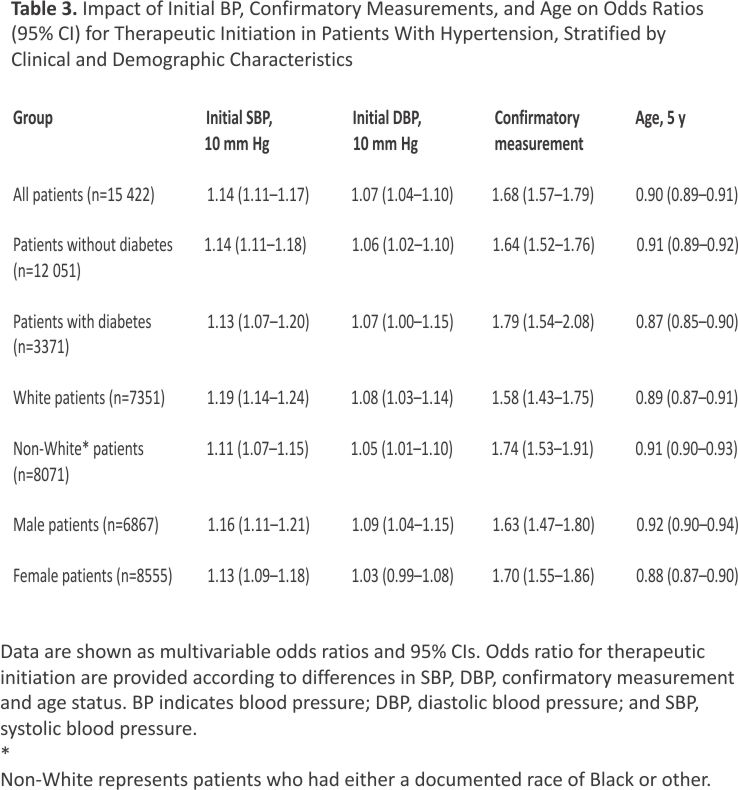
The likelihood of TI during the first month after the diagnosis of hypertension was 14% greater for each 10 mm Hg increment in SBP and 7% higher for each 10 mm Hg increment in DBP, adjusting for age, race, sex, and diabetes (Table 3). No significant interaction terms were found. The effect of SBP and DBP on TI was similar in groups by diabetes, race, and sex status. Confirming SBP ≥140 on repeated measurement(s) during the initial visit increased the likelihood of TI by ≈68%, with similar effects in groups defined by age, race, sex, and diabetes status. Each 5-year increment in age reduced the likelihood of TI by roughly 10%, with similar effects in groups defined by sex, race, and diabetes status.
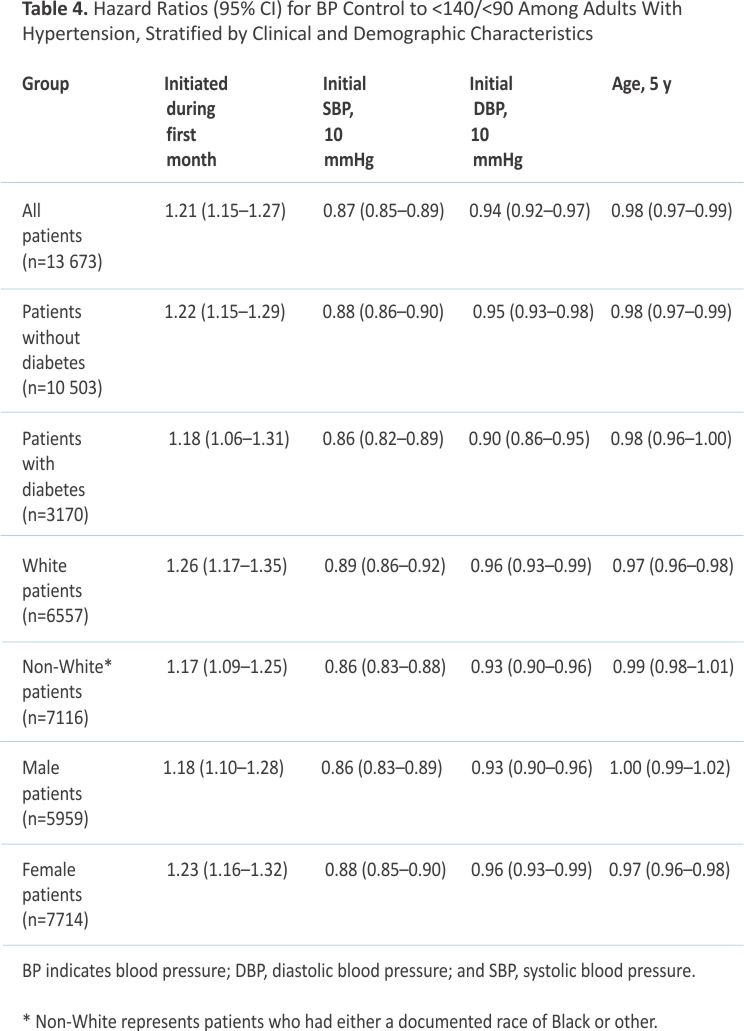
BP control during the 42-month follow-up period was 19% more likely for patients with TI during the first month (hazard ratio [HR], 1.19 [95% CI, 1.13–1.25]) than patients untreated during the first month, which persisted after adjusting for age, race, sex, and initial SBP (HR, 1.21 [95% CI, 1.15– 1.27], Table 4). The benefit of TI in the first month after diagnosis of hypertension was also observed for the control threshold of <130/<80 mmHg after multivariable adjustment (HR, 1.14 [95% CI, 1.07–1.21]).
DISCUSSION
The principal finding of our study is that patients with untreated, uncontrolled hypertension who are initiated on monotherapy during the first month following the diagnosis of hypertension achieved better BP control at 6 months than patients who were not treated in the first month. Hypertension control within the first 6 months of treatment reduces the incidence of cardiovascular events.1–5 Moreover, superior control was maintained through 30 months in the group with TI in the first month, compared to later time points.
Treatment with initial mono-therapy was the focus, since most adults with hypertension are initiated on a single antihypertensive medication class.8,12,13 While initial monotherapy predominates, initial combination therapy leads to better BP control 12,15, fewer cardiovascular events,8,18 and is recommended in the treatment guidelines.7,18
In our study, the cumulative rate of TI increased as a function of time (Figure 2), whereas the rate of increase slowed over the course of 42 months (Figure 2). For patients initiated on monotherapy, subsequent treatment intensification is often required to attain BP control.7,18,20–22 However, patients initiated on monotherapy in the first month did not achieve 70% or higher control rates to <140/<90. This finding is consistent with their low rates of subsequent therapeutic intensification for uncontrolled hypertension, which averaged ≈16% at 6 months, 14% at 12 months, and roughly 10% thereafter (Figure S1). Our findings coincide with other reports that treatment intensification occurs in <1 in 6 encounters when BP is uncontrolled and represents a key barrier to good BP control.19–21
Regression toward the mean is a phenomenon wherein a group of individuals selected for high or low values on biological variables, for example, BP, regress toward mean values over time.22,23 This phenomenon may contribute to the decline of mean SBP in patients not treated during the first month after diagnosis, as well as in patients who were initially treated. The group treated during the first month after diagnosis experienced a greater decline in SBP than the untreated at 6 months (17.1 versus 12.4 mm Hg), providing evidence for the effectiveness of initial monotherapy in lowering BP and improving control. In multivariable analysis, patients with TI during the first month had a 21% greater likelihood of control to <140/<90 (HR, 1.21 [95% CI, [1.15–1.27]) across the 42-month study period, supporting the relationship between prompt treatment and time to BP control (Table 4). TI during the first month after diagnosis also improved control to <130/<80 (HR, 1.14 [95% CI, 1.07–1.21]).
The population mean SBP of ≈135 in this study is comparable to that in the SPRINT standard treatment group, where control rates to <140/<90 were ≈60%.18 Evidence indicates that a mean SBP <130 is required to control 80% or more of patients to <140/<90, which suggests that greater rates of antihypertensive treatment intensification are required to attain higher rates of control.24,25 Estimates suggest that treatment intensification would need to occur on at least 5 of 8 visits with uncontrolled BP to improve control rates from 46% to 80% or higher.19
Our study highlights key variables associated with higher rates of TI. Higher SBP and DBP increased, while ageing reduced the likelihood of TI. Of note, a repeat BP measurement confirming uncontrolled BP increased the likelihood of TI by over 60%, an effect which was similar across groups defined by diabetes, race, and sex (Table 3). Guidance to repeat the measurement of BP following an uncontrolled reading is an established feature of quality improvement programs, including Kaiser Permanente and AMA MAP Hypertension.11,26 Confirmatory measurements partially address the concern of inaccurate and nonrepresentative BP values, which contribute to therapeutic inertia.20
Limitations of this study include reliance on electronic health record data, which are often incomplete and inconsistent, especially with interoperability challenges when integrating data from multiple heterogeneous health care organisations with differing information systems and documentation practices. When relying on real-world data systems, information potentially relevant to the scope of the study for patients receiving health care services at external locations is not available. Our database is dependent on the integrity of data extracted from electronic health record systems and data warehouses, with limited capabilities for validation against source documents. Further, numerous errors occur during BP measurement in usual care settings. 27 BP values are occasionally entered in a text field note, and our database includes only values in the vital signs fields. Information on prescribed medications is often incomplete or erroneous, depending on accurate and timely medication reconciliation, which includes medications prescribed by clinicians using different electronic health record systems.28 Our study period included the COVID pandemic, during which in-person visits, typically including BP values, declined, and virtual visits, less often tracking relevant patient vitals, increased.29 Further, while evaluating the risk of cardiovascular events as a function of the time to treatment initiation was of interest, the data to assess clinical outcomes was not reliably available.
Our study addressed some limitations through data cleaning and validation methods used by the MAP Hypertension program, which requires a higher standard of encounter, medication, and diagnostic documentation complete- ness. Patients included in the analysis were required to have an outpatient visit history within the organisation before their initial hypertension diagnosis, reducing the likelihood of erroneous inclusion from incomplete history.
In summary, TI during the first month after the diagnosis of hypertension leads to better hypertension control for 30 months than delayed beyond the first month.
PERSPECTIVES
Adults with untreated and uncontrolled hypertension are more likely to achieve BP control to <140/<90 in the first 6 months after diagnosis when antihypertensive monotherapy is initiated during the first month of diagnosis than at later time points. Moreover, improved control was sustained for 30 months following diagnosis in this initially treated group compared with the group that was not treated in the first month after diagnosis. While patients initiated on monotherapy during the first month following diagnosis of hypertension achieved higher control rates than individuals initiated at later time points, >30% remained uncontrolled at 3 years, indicating a need for more frequent treatment intensification. Confirming an uncontrolled BP during the visit was associated with a greater probability of treatment initiation. Importantly, hypertension control during the first 6 months after diagnosis provides greater cardiovascular protection than delayed control.
Acknowledgments
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the American Medical Association.
Affiliations
Robert B. Barrett – American Medical Association, Greenville, SC
Benjamin Riesser – American Medical Association, Greenville, SC
Benjamin Martin – Johns Hopkins University, School of Medicine, Baltimore
Neha Sachdev – American Medical Association, Chicago, IL
Michael K. Rakotz – American Medical Association, Chicago, IL
Susan E. Sutherland – American Medical Association, Greenville, SC
Brent M. Egan – American Medical Association, Greenville, SC
Footnote
Nonstandard Abbreviations and Acronyms
AMA – American Medical Association
BP – blood pressure
DBP – diastolic blood pressure
HR – hazard ratio
ICD-10-CM – International Classification of Diseases, Tenth Revision, Clinical Modification
MAP – Measure Accurately, Act Rapidly, Partner with Patients
SBP – systolic blood pressure
TI – treatment initiation
References
1. Martin-Ferna´ndez M, Vinyoles E, Real J, Soldevila N, Munoz MA, DelVal JL, Verdú JM, Domingo M, Mundet X. The prognostic value of blood pressure control delay in newly diagnosed hypertensive patients. J Hypertens. 2019; 36:426-431. doi: 10.10 97/HJH. 0000000000001896
2. Julius S, Kjeldsen SE, Weber M, Brunner HR, Ekman S, Hansson L, Hua T, Laragh J, McInnes GT, Mitchell L, et al; VALUE Trial Group. Outcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the VALUE randomised trial. Lancet. 2004;363:2022–2031. doi:10. 1016/S0140-6736(04) 16451-9
3. Laiteerapong N, John PM, Meltzer DO, Huang ES. Impact of delaying blood pressure control in patients with type 2 diabetes: results of a decision analysis. J Gen Intern Med.2011;27:640-646. doi: 10.1007/s11606-011-1951-y
4. Staessen JA, Thijs L, Fagard R, Celis H, Birkenhäger WH, Bulpitt CJ, de Leeuw PW, Fletcher AE, Forette F, Leonetti G, et al; Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Effects of immediate versus delayed antihypertensive therapy on outcome in the Systolic Hypertension in Europe Trial. J Hypertens. 2004; 22:847-857. doi: 10.1097/0000 4872-2004 04000-00029
5. Miriampillai JE, Eskas PA, Heimark S, Kjeldsen SE, Narkewwicz K, Mancia G. A case for less intensive blood pressure control: it matters to achieve target blood pressure early and sustained below 140/90 mmHg. Prog Cardiov Dis. 2016; 59:209-218. doi:10.1016/j.pcad. 2016.09.002
6. Quality ID #236 (NQF 0018): Controlling high blood pressure. Dec 2021. https://qpp.cms.gov/ docs/QPP_quality_measure_specifications/Claims-Registry-Measures /2022_Measure_236_MedicarePartBClaims.pdf.
7. Whelton PK, Carey RM, Aronow WS, Casey DE, Collins KJ, Dennison Himmelfarb C, DePalms SM, Gidding S, Jamerson KA, Jones DW, et al. 2017 ACC/AHA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults. Hypertension. 2018;71:e13–e115.
8. Rea F, Corrao G, Merlino L, Mancia G. Initial antihypertensive treatment strategies and therapeutic inertia: evidence from a large population-based cohort. Hypertension. 2018; 72: 846–853. doi: 10.1161/ HYPERTENSIONAHA.118.11308
9. De Backer T, Van Nieuwenhuyse B, De Bacquer D. Antihypertensive treatment in a general uncontrolled hypertensive population in Belgium and Luxembourg in primary care: therapeutic inertia and treatment simplification. The SIMPLIFY study. PLoS One. 2021; 16:e024 8471. doi: 10.1371/journal.pone. 0248471
10. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370:1453–1457. doi: 10. 1016/S0140-6736(07)61602-X
11. Egan BM, Sutherland S, Rakotz M, Yang J, Hanlin RB, Davis R, Wozniak G. Improving hypertension control in primary care with the Measure accurately, Act rapidly and Partner with patients (MAP) Protocol: Results at 6 and 12 months. Hypertension. 2018;72:1320 –1327. doi: 10. 1161/HYPERTENSIONAHA. 118.11558
12. Smith SM, Winterstein AG, Gurka MJU, Walsh MG, Keshwani S, Libby AM, Hogan WR, Pepine CJ, Cooper-DeHoff RM. Initial antihypertensive regimens in newly treated patients: real world evidence from the OneFlorida+C Clinical Research Network. JAHA. 2022;11:e026652. doi: 10.1161 /JAHA.122.026652
13. Egan BM, Bandyopadhyay D, Shaftman SR, Wagner CS, Zhao Y, Yu-Isenberg KS. Initial mono- and combination therapy and blood pressure control in the first year. Hypertension. 2012; 59:1124–1131. doi: 10.1161/HYPERTENSIONAHA. 112.194167
14. Feldman RD, Zou GY, Vandervoort MK, Wong CJ, Nelson SA, Feagan BG. A simplified approach to the treatment of uncomplicated hypertension: a cluster randomized, controlled trial. Hypertension. 2009; 53:646–653. doi: 10.1161 /HYPERTENSIONAHA. 108.123455
15. Chow CK, Atkins ER, Hillis GS, Nelson MR, Reid CM, Schlaich MP, Hay P, Rogers K, Billot L, Burke M, et al: QUARTET Investigators. Initial treatment with a single pill containing a quadruple combination of quarter doses of blood pressure medicines versus standard dose monotherapy in patients with hypertension (QUARTET): a phase 3, randomised, double-blind, active-controlled trial. Lancet. 2021;398:1043–1052. doi: 10.1016/S0140-6736(21)01922-X
16. Rodgers A, Salam A, Schutte AE, Cushman WC, de Silver HA, Di Tanna GL, Grobbee DE, Narkiewicz K, Ojji DB, Poulter NR, et al. Efficacy and safety of a novel low-dose triple single-pill combination of telmisartan, amlodipine and indapamide, compared with dual combinations for treatment of hypertension: a randomised, double-blind, active-controlled, international clinical trial. Lancet. 2024;404: 1536–1546. doi: 10.1016/S0140-6736(24)01744-6
17. Rea F, Corrao G, Merlino L, Mancia G. Early cardiovascular protection by initial two-drug fixed-dose combination treatment vs. monotherapy in hypertension. Eur Heart J. 2018;39:3654-366. doi: 10.1093/eurheartj/ehy420
18. Mancia G, Kreutz R, Brunström M, Burnier M, Grassi G, Januszewicz A, Muiesan ML, Tsioufis K, Agabiti-Rosei E, Engi AEA, et al. 2023 ESH Guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension. J Hypertension. 2023;41:1374-2071. doi: 10.1097/ HJH.00000 00000003480
19. Bellows BK, Ruiz-Negrón N, Bibbins-Domingo K, King JB, Pletcher MJ, Moran AE, Fontil V. Clinic-based strategies to reach United States Million Hearts 2022 blood pressure control goals: a simulation study. Circ Cardiovasc Qual Outcomes. 2019; 12:e005 624. doi: 10.1161/CIRCOUTCOMES.118.005624
20. Ali DH, Kiliç B, Hart HE, Bots ML, Biermans MCJ, Spiering W, Rutten FH, Hollander M. Therapeutic inertia in the management of hypertension in primary care. J Hypertens. 2021; 39:1238-1245. doi: 10.1097/ HJH.0000000000 002783
21. Okonofua EC, Simpson K, Jesri A, Rehman S, Durkalski V, Egan BM. Therapeutic inertia is an impediment to achieving Healthy People 2010 blood pressure control goals. Hypertension. 2006;47:1–7. doi:10. 1161/01. HYP.0000200702. 76436.4b
22. Linden A. Assessing regression to the mean effects in health care initiatives. BMC Med Res Methodol. 2013;13:119. doi: 10.1186/1471-2288-13-119
23. Wang N, Atkins ER, Salam A, Moore MN, Sharman JE, Rodgers A. Regression to the means in home blood pressure: analysis of the BP GUIDE study. J Clin Hypertension. 2020;22:1184–1191. doi:10. 1111/ jch.13933
24. The SPRINT Research Group. A randomised trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373: 2103–2116.
25. Egan BM, Li J, Wagner CS. Systolic blood pressure intervention trial (SPRINT) and target systolic blood pressure in future hypertension guidelines. Hypertension 2016;68: 318 –323. doi: 10.1161/HYPER-TENSIONAHA.116.07575
26. Jaffe MG, Young JD, Sidney S, Go AS. Improved blood pressure control associated with a large-scale hypertension program. JAMA. 2013;310:699–705. doi: 10.1001/ jama.2013.108769
27. Muntner P, Shimbo D, Carey RM, Charleston JB, Misra S, Myers MG, Ogedegbe G, Schwartz JE, Townsend RR, Urbina EM, et al. Measurement of blood pressure in humans: a scientific statement from the American Heart Association. Hypertension.2019; 73:e35–e66. doi: 10.1161/HYP.0000000000000087
28. Rangachari P, Dellsperger KC, Fallaw D, Davis I, Sumner M, Ray W, Fiedler S, Nguyen T, Rethemeyer RK. A mixed-method study of practitioners’ perspectives on issues related to EHR medication reconciliation at a health system. Qual Manage Health Care. 2019;28:84-95. doi: 10.1097 /QMH.0000000000000208
29. Alexander GC, Tajanlangit M, Heyward J, Mansour O, Qato DM, Stafford RS. Use and content of primary care office-based vs telemedicine care visits during the COVID-19 pandemic in the US. JAMA Netw Open. 2020;3:e2021476. doi: 10.1001 /jamanetworkopen.2020.21476