

Abdulsamad Salihu, Ibrahim Jahun, David Olusegun Oyedeji, Wole Fajemisin, Omokhudu Idogho, Samira Shehu, Aminu Yakubu & Jennifer Anyanti
Abstract
Over the years, Nigeria has recorded significant progress in controlling the HIV epidemic in the country. HIV prevalence has reduced from 4.1% in 2010 to 1.4 in 2019. The number of people acquiring new HIV infections decreased from 120,000 in 2010 to 74,000 in 2021, and HIV-related deaths decreased from 82,000 in 2010 to 51,000 in 2021. However, the country still faces challenges such as high HIV transmission among key populations (KP) who account for 11% of new HIV infections. Over the years, the government and development partners involved in HIV response efforts in Nigeria have been establishing and scaling up access to services to help address the needs of KPs. Initially, services for KPs as with the general population in Nigeria were largely preventive. Treatment of PLHIV in Nigeria commenced in 2002 and has increased from about 15,000 to more than 1.78 million PLHIVs in 2023. Despite this progress in treatment coverage, however, KPs are not equitably covered. To address this gap, the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) launched an ambitious initiative—the Key Population Investment Fund (KPIF)—to target the unaddressed HIV-related needs of key populations (KPs) who are disproportionately affected by HIV. The KPIF initiative was implemented through partner organizations such as the Society for Family Health (SFH), a KP-friendly and indigenous non-governmental organization. Earlier, the program implemented by SFH was largely an HIV prevention program. SFH’s transformation, transition, and growth to a comprehensive HIV prevention, care, and treatment service provider was necessary to bridge the gap in the needed expansion of HIV services to adequately meet the care needs of KPs and scale up programs. Therefore, this paper’s aim is to share experiences in the transformation of SFH into a comprehensive HIV prevention, treatment, and care service provider in the hope that it may serve as a lesson for organizations with similar objectives.
Introduction
Globally, the world has made significant progress towards controlling the Human Immuno- deficiency Virus (HIV) epidemic with a 52% reduction in HIV-related deaths—from 1.3 million [970 000–1.8 million] in 2010 to 630 000 [480,000–880,000] in 2022 1. The number of people becoming newly infected with HIV has dropped by 38% to 1.3 million [1.0–1.7 million], from 2.1 million [1.6–2.8 million] in 2010 1. Despite its disproportionate burden of HIV, with two-thirds of all people living with HIV, Africa has also recorded significant progress in controlling HIV on the continent. HIV-related deaths have reduced by 55.8% to 380,000 deaths in 2022 from 860,000 in 2010. New HIV infections have also reduced by 56% to 660,000 [480,000–920,000] in 2022 compared to 2010 2. However, HIV continues to be a major global public health issue. In 2022, there were 39.0 million [33.1–45.7 million] people living with HIV, 1.3 million [1.0–1.7 million] people became newly infected, and 630,000 [480,000–880,000] people died from HIV-related causes globally 1,2.
Although the West and Central African region has the lowest rates of HIV in Africa, Nigeria, with about 1.9 million people living with HIV, is one of the top five countries that account for the highest number of HIV-positive people in the world 3. Over the years, Nigeria has also recorded significant progress in controlling the HIV epidemic in the country. HIV prevalence has reduced from 4.1% in 2010 to 1.4 in 2019. The number of people acquiring new HIV infections decreased from 120,000 in 2010 to 74,000 in 2021, and HIV-related deaths decreased from 82,000 in 2010 to 51,000 in 2021 4.
There are significant gaps that remain for the world and Nigeria to attain the globally accepted UNAIDS 95-95-95 targets. These are ambitious targets that seek to ensure that by the year 2025, 95% of all people living with HIV know their HIV status, 95% of all people with HIV infection receive sustained antiretroviral therapy, and 95% of all people receiving antiretroviral therapy have viral suppression. As of 2022, the global 95-95-95 status was estimated at 86–76–71% respectively 1—indicating significant gaps in global progress towards attaining the targets. Nigeria’s progress towards the UNAIDS 95-95-95 targets has improved to 90-90-86, bringing the country remarkably closer to epidemic control 5. However, the country still faces challenges of high HIV transmission among key populations (KP) 5,6.
Globally, HIV is disproportionately higher among KPs, which comprises gay men and other men who have sex with men (MSM), sex workers (SW), people who inject drugs (PWID), and transgender people (TG). In 2022, HIV prevalence among MSM, SW, PWID, and TG, was 11, four, seven, and 14 times more than in the general population respectively 1. In Nigeria, data from the 2020 Integrated Behavior and Biological Seroprevalence Survey (IBBSS) showed that KPs account for 11% of new HIV infections. KP-subpopulations have a higher HIV prevalence (10.9% for PWID, 15.5% for SW, 25.0% for MSM, and 28.8% for TG) compared to the general population (1.3%)7.
In Nigeria and other countries, HIV among KPs is fueled by stigma and discrimination, repressive laws and policies and criminalization of behaviors. In terms of stigma, it is estimated that at least 42% of all KP populations have been forced to have sex because of their orientation, and at least 16.5% have been harassed or arrested by law enforcement agents 7. On the other hand, the ‘Same Sex Marriage Prohibition Act’ 8 enacted in 2014 criminalizes all activities related to same-sex sexual relationships, including marriage, meetings, and provision of healthcare services 9. Consummating same-sex marriage is punishable by 14 years imprisonment. While participating in gay meetings or public show of same-sex relationship, or supporting such marriages or meetings are punishable by 10 years imprisonment 8. Collectively, stigma, discrimination and criminalization of KP behaviors tend to deter or restrict access of KPs to health services and thereby increase their vulnerability to HIV and other diseases 10,11,12,13,14,15,16. Given the disproportionately higher HIV and the limited coverage of services among KPs, attaining epidemic control is only feasible if HIV is effectively controlled among this population. This requires innovative mechanisms to address the demand and supply side challenges militating against the provision of quality HIV prevention, treatment, and care services to KPs.
The Society for Family Health (SFH), initially an HIV prevention services provider, reformed and expanded into a comprehensive HIV prevention, treatment, and care service provider to help address this need. In this paper, we share experiences about this transformation process as a lesson for organizations with similar objectives.
SFH HIV services expansion and transformational journey
Historical reach and focus, pre-transformation
In the early days of HIV in Nigeria and other developing countries, the focus of control efforts was on prevention. This typically included behavioral change communication (BCC) and condom promotion and distribution initiatives. The impact of such strategies was however minimal, perhaps due to poor adherence to the strategies promoted, such as abstinence, faithfulness to one uninfected sexual partner at a time, and correct and consistent condom use. Denials, myths, and misconceptions about HIV were major contributors to poor uptake of the prevention initiatives thus leading to the propagation of HIV in developing countries, especially, African countries. Established in 1983, SFH was already a major player in condom programming in Nigeria—helping to promote condom use as a family planning strategy towards improving the contraceptive prevalence rate in the country when HIV was first diagnosed in Nigeria 3 years later 17. Some of the projects through which SFH provided these Sexual and Reproductive Health services included Promoting Sexual Reproductive Health and HIV Prevention (PSRHH) program 18, the promotion of Universal Access to Female Condom (UAFC) project, Enhancing Nigeria’s Response to HIV program (ENR) 19 and the Expanded Social Marketing Project in Nigeria (ESMPIN) 20.
The expansion of SFH’s health promotion and family planning services to include HIV can arguably be traced back to 2002, through the project Promoting Sexual Reproductive Health (PSRHH) (2002 –2006). In this project, SFH developed the Peer Education Plus (PEP) model which combined multiple aspects of behavior change communications, advocacy visits, open community meetings, peer education sessions, drama, IEC materials and product distribution, condom and condom lubricant distribution, and referral for HIV testing and STI treatment, to promote responsible behaviors that help to control the spread of HIV. One critical component of the PEP was the deliberate efforts to build a sustainable aspect to the program through the nurturing of hundreds of community-based organizations to sustain activities of the program after it ends and to scale up prevention activities. The key messages in the PEP include partner reduction, correct and consistent condom use in all sexual acts, primary and secondary abstinence, prompt and complete treatment of sexually transmitted infections (STIs), and testing for HIV. Other important HIV prevention projects implemented by SFH include the USAID-funded Comprehensive Integrated Approach to HIV/AIDS Prevention and Care in Nigeria (CIHPAC) from 2006 to 2010. Through CIHPAC, SFH and partners reached more than three million individuals with behavior change communications and provided HIV counseling and testing to over 150,000 individuals, contributing to the reduction in HIV prevalence recorded in that period, from 4.5% in 2005 to 4.1% in 2011 21. The program also nurtured, supported, and enhanced the capacity of many Community-Based Organizations (including Faith-Based Organizations and local NGOs) 22. The Enhancing Nigeria’s Response to AIDS (ENR) program (2009–2014) worked with 7 states in Nigeria and through their efforts helped to enact anti-stigma and discrimination laws in these seven (7) states, which then were the only states in Nigeria with such laws at the end of the project in 2014 23. The project distributed 1.2 billion male and 4.0 million female condoms in 6 years.
Since 2010, with funding from the Global Fund to Fight AIDS, TB, and Malaria (GFATM), SFH has implemented HIV prevention programs in 13 states that include BCC, HCT, referral and linkage to treatment for KPs who test positive, as well as the provision of comprehensive HIV and STDs syndromic management services. In 2017 alone SFH reached 161,106 KPs with prevention interventions, tested 120,897, and identified 5234 new positives of which 4202 were successfully placed on treatment through its GFATM portfolio.
Also, from 2009 to 12 through the CIHPAC project, SFH commenced syndromic management, through Drop-in Centers (DICs) and continued this with the SHiPS for MARPs project in 2013 and then intensified with the creation of One Stop Shops (OSS) in 2015 across 7 states for treatment services for KPs and have since sustained this service until the SHiPS project ended in 2018.
Expansion of HIV treatment program in Nigeria
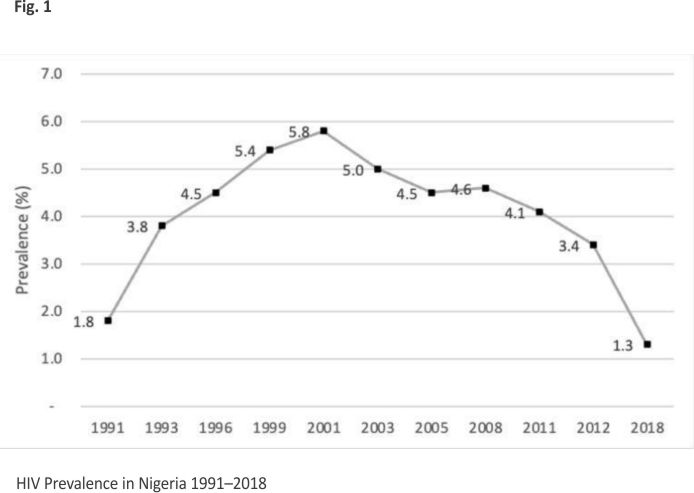
Initially, services for KPs as with the general population in Nigeria and other developing countries were largely preventive 24. With a prevention-only strategy, and a culture of denial, myths, and misconceptions, Nigeria’s HIV prevalence grew over the years. From the two HIV cases reported in 1986 25, Nigeria’s HIV prevalence grew from 1.8% in 1991 and reached a peak of 5.8% in 2001 21. However, perhaps by some work of providence, the year 2001 marked a watershed moment for the control of HIV in Nigeria. Following the United Nations General Assembly Special Session on HIV/AIDS in 2001, at which member countries adopted a declaration to control HIV/AIDS, Nigeria also pledged to launch an ARV program to stem the tide of HIV in the country. Treatment of PLHIV in Nigeria commenced in 2002 26 in 25 tertiary health facilities aimed at reaching 10,000 adults and 5000 children. The government’s initiative was soon complemented by the launch of the HIV control initiatives that also focused on treatment saturation by the United States PEPFAR program (2004 till date) 27 and the GFATM (2005 till date) 4. Following the launch of the HIV treatment program in Nigeria in 2001 and subsequent treatment programs, PEPFAR and GFATM showed demonstrable impact over the years. The prevalence of HIV, which peaked at 5.8% in 2001, gradually fell to 4.1% in 2010, and 3.4% in 2013 and reached its lowest of 1.4% in 2018 21 as illustrated in Fig. 1.
 Despite the existence of the HIV treatment program, Nigeria’s progress to attain the globally accepted UNAIDS 90-90-90 target for HIV treatment was consistent but slow over the years. According to this target, for treatment, countries were expected to have placed 90% of PLHIV who know their status on treatment by the year 2020. However, as of 2015, only 5 years to the target, Nigeria had met only 50% of this target.
Despite the existence of the HIV treatment program, Nigeria’s progress to attain the globally accepted UNAIDS 90-90-90 target for HIV treatment was consistent but slow over the years. According to this target, for treatment, countries were expected to have placed 90% of PLHIV who know their status on treatment by the year 2020. However, as of 2015, only 5 years to the target, Nigeria had met only 50% of this target.
The U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) launched an ambitious initiative — the Key Population Investment Fund (KPIF)—to target the unaddressed HIV-related needs of key populations (KPs) who are disproportionately affected by HIV, strategically in 2016, and operationally in 2019 10. The success of the KPIF was hinged on the ability of PEPFAR to partner with organizations that can provide comprehensive prevention and treatment services for KP. The KPIF initiative was implemented by USAID and CDC through partner organizations. SFH was one of the partners that worked with USAID in the KPIF and initially focused on HIV prevention. However, SFH’s transformation to a comprehensive HIV prevention, care, and treatment service provider was necessary to meet the care needs of KPs.
This seemed to be a pragmatic decision, given the organization’s presence in more than 20 of the 36 states and the FCT Abuja and the availability of Drop-In Centers for HIV prevention, testing, and counseling services, which can be transformed into treatment facilities with minimal restructuring.
As the world approaches HIV epidemic control with cautious optimism, ensuring adequate treatment coverage for KPs remains crucial. Increasing the number of organizations providing high-quality, innovative, KP-friendly services could help overcome extant barriers to KP service provisioning 28.
SFH transition to a comprehensive HIV prevention, care, and treatment provider
In October 2016, SFH transitioned to a comprehensive HIV prevention, care, and treatment service provider with the SHiPS for MARPS Project, although this decision was taken earlier in 2015. This shift in programming was in line with the PEPFAR High Impact Agenda and the UNAIDS 90-90-90 targets. To actualize this transition, some organizational reforms to ensure that the known barriers to accessing HIV treatment among KPs were overcome became imperative. These included health systems, capacity, client, and community-related barriers 29. Health system-related barriers that the reforms aimed to address include poor treatment literacy, long waiting times, rigid hours for service provision, the high out-of-pocket cost for ART, inadequate health infrastructure, limited availability of ART medications, social stigma and discrimination from health care workers, and absence of person-centered approach to care at health facilities 30,31.
Regarding capacity-related barriers, the reforms incorporated continuous capacity-strengthening initiatives such as periodic training, workshops, and mentorship aimed to ensure service provider understanding of KP service provision barriers and extant ART provision guidelines for KP including HIV testing options and rapid ART initiation in line with the World Health Organization’s consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring 32. For the Client-related barriers, SFH’s transition aims to address issues related to financial barriers to treatment access, and challenges of transportation to facilities, as well as fear of adverse drug effects, and the stigma associated with HIV, which are already being addressed under the comprehensive prevention package 33. The reforms would also deepen community-related obstacles including the criminalization of same-sex relationships, and societal stigma and discrimination against KPs 34,35. To address the health system barriers to HIV treatment for KPs, two approaches were deployed— the establishment of One-stop shops (OSS), and the institutionalization of KP-friendly service culture into existing ART health facilities. The OSSs are innovative models for providing full-spectrum services in the HIV prevention, care, and treatment cascade. Services available at these OSSs often also address non-health-related issues and other barriers to care to address the needs specific to KPs. These include legal support services to help with harassment by law enforcement, and economic empowerment support to help with good nutrition and transportation costs to access care among others 36. The OSS model is the most widespread of three models for community-based ART that various stakeholders in Nigeria have deployed to improve access to treatment for KPs. The other two models include community drop-in-centers (DIC), and community ART outreach 30,37. SFH team also worked very hard to ensure that internal staff, external consultants, and state and community implementing partners received the necessary capacity development and supervisory/mentoring support needed to manage this transition and deliver adequately.
In the first year of the transition from largely a prevention program to a treatment and care support program, SFH started by establishing the OSSs. To leverage on existing structures and systems, SFH upgraded seven of the 12 Drop-in Centers it had set up under the SHiPs for Marps project to One-Stop Shops (OSS). This included staff recruitment to strengthen the existing team, setting up a laboratory for all necessary clinical evaluations needed to enable informed initiation of ART, and remodeling to provide adequate space for clinical consultations, counseling, HTS, and other required services. The SFH team then designed and equipped a comfortable waiting room/recreational area which enabled KPs to have a safe area where they could seek counseling and social support with-out feeling self or enacted stigma which was high at the time. The space was available for KPs, even if they were not accessing clinical services, and helped identify and mobilize KPs yet to uptake available services. This feature was a great selling point for the OSS among project beneficiaries. In the second year, 2017, an additional seven OSSs (one in each state) were established to address the increase in client numbers as well as the challenge of distance to the initial OSS for some project communities in seven (7) States (Lagos, Rivers, Akwa Ibom, Benue, Cross-rivers, Nassarawa, and FCT Abuja). Other states within other SFH programs maintained the drop-in centers.
Stigma and discrimination from healthcare workers are key barriers to care access for KPs 38. To ensure optimal service delivery at the newly established OSSs, key health-care workers were recruited, trained, and deployed at each of the OSSs. These include at least one medical doctor, who serves as the clinical supervisor, then a pharmacist, laboratory scientist, triage Nurse, community nursing officer, and medical records officer, among others. All staff received training on ART provision, client-centered care, stigma-free service delivery, and logistics management of HIV commodities. The project also expanded the pool of Case Management Officers (CMOs) to strengthen successful enrolment into ART and sustained adherence counseling for positive peers. CMOs are trained to manage cohorts of HIV-positive peers and provide continuous client follow-up, counseling, and support until viral suppression is achieved. By their design, OSSs also provide services that help to address client-centered barriers to care, such as self-stigma, lack of funds to access ART, and transportation to the ART service points 37. The OSS we established, in addition to comprehensive health services along the entire HIV continuum of care, also provided psychosocial counseling and support with finances and transportation needs for the clients. A critical success factor for the team is the use of the SFH core team which included a state program manager and his/her team to ensure mobilization of KPs, advocacy and ensuring an enabling environment, communicating and working with the state gatekeepers to ensure scale up and ownership of the project, coordinating with the CBOs and other implementing groups, documentation, monitoring and evaluation and ensuring accountability.
For existing ART health facilities, identification, and selection for transformation into KP-friendly ART health facilities was done in collaboration with the KP community members, CSOs/CBOs, and State Ministries of Health. Fifty-four facilities across 9 states (Lagos, Oyo, Anambra, Imo, Edo, Gombe, Kano, Enugu, and Abuja) were selected. All states were selected based on epidemio-logical and empirical evidence and the need to prioritize interventions within a defined geographical location to achieve maximal impact. States were selected because they are estimated to have a high number of KPs based on existing KP size estimation studies and/or the Integrated Biological and Behavioral Sero Surveillance (IBBSS) studies. Staff at the existing ART health facilities were trained on the provision of KP-friendly services to KPs, some health care providers were also trained on syndromic Management of Sexually Transmitted Infections (STIs), comprehensive human sexuality education, HIV pre-and post-test counseling; safer sex/ risk-reduction counseling, condom promotion, and interventions targeted at key populations. In addition, Community-based HIV Counsellor Testers were engaged (some are members of the KP community) and trained to screen KPs for HIV and accompanied those who screened positive for HIV, TB, and STI to the friendly health facilities and ensure rapid initiation on ART and provision of STI Syndromic Management and treatment. Involving KPs at levels of service update and as implementing partners promoted ownership, allowed for co-creation and co-design of approaches to address any gaps or challenges, and promoted accountability.
The 2023 World AIDS Report has given a new impetus to the role of communities in ending the HIV epidemic globally 1. The report’s emphasis on community-led HIV interventions is at the heart of the community-based ART models including the OSS model. These models promote the engagement of local and KP communities to design and locate the services appropriately to avoid societal disruptions. KPs also play important roles in providing services through these community ART models. These include peer HIV counseling and testing, accompanied referral, tracking of clinic defaulters by peers and network, provision of condoms, and KP sensitization for HCWs among others 30.
Setting up the OSS and KP-friendly facilities starts with consultations with key stakeholders in each state. These include representatives of the authorities responsible for oversight of efforts to control AIDS at the local government and state levels. These are called Local Action Committees on AIDS (LACAs) and State Agencies for the Control of AIDS (SACAs) respectively. In addition, consultations also involved representatives of civil society organizations active in HIV control efforts, specifically, the KP-led organizations and organizations that are championing the care needs of KPs. Consultations with the Ministries of Health in the States, representatives of LACAs, SACAs, and religious and traditional leaders, ensure buy-in of these important gatekeepers of the initiatives and facilitate consensus on suitable locations to site the facilities for the OSSs and the selection of ART health facilities for the KP-friendly transformation approach. It is also an important step to ensure alignment of the OSS and the KP-friendly facilities into the overall AIDS control plan of the state as this promotes sustainability and enhanced engagement with policy issues needed to address stigma, discrimination, and neglect of the needs of KPs. Consultations with civil society organizations active in HIV control efforts, especially those that are KP-led also enabled buy-in as well as agreement on the role of the KP representatives in the operations of the OSS and the KP-friendly facilities, and identification of suitable KP candidates to take on available positions and training, especially in the OSSs. Figure 2 high-lights some of the key considera- tions in SFH’s transformation from a prevention-only, to a comprehensive HIV service provider.
![]() The design of the OSS and KP-friendly facilities ensured that both initiatives could provide services for all KP groups—SW, MSM, PWID, and TG alike, thereby ensuring inclusivity.
The design of the OSS and KP-friendly facilities ensured that both initiatives could provide services for all KP groups—SW, MSM, PWID, and TG alike, thereby ensuring inclusivity.
Successes, challenges, and way forward
Our organization’s transition to a comprehensive, prevention, care, and treatment partner began in 2015 and 2016 with the Global Fund New Funding Model (2015–2017) and the USAID-funded SHiPS for MARPs respectively showed remarkable results. For example, data from the SHiPS for MARPs project showed that between 2016 and 2017, 4532 HIV-positive KPs were identified, out of which 93% were placed on ART. Thus, we achieved 170% of the projects’ combined target for positive KPs identified and 430% of the target for the number of KPs initiated on ART. Out of 4532 positive KPs identified in USAID focal states, 4029 (93%) were initiated on ART, and 3909 out of 4029 (93%) initiated on ART were still on ART. This compares to findings from a similar KP program in Benue State, supported by APIN Public Health Initiatives, a pioneer in comprehensive HIV services provision in Nigeria. The APIN program enrolled 3945 KP between 2016 and 2019, with 65.3% retention rate in the first year of enrolment 30. Arguably, the successes of our comprehensive program resulted in the award of an extension of the Global Fund NFM grant for another 2 years, 2018–2019, and a new USAID award for KP, the Key Population Community HIV Services for Action and Response (KP CARE 2) (2019–2024). Both awards are focused on expanding access to treatment for KPs within a comprehensive prevention, care and treatment program.
At the states where these projects were implemented such as Lagos, Akwa Ibom and FCT, we have noted that these states have evolved with a capacity to pitch and win grants as principal recipients for GF and other grants to enable them to expand the treatment and care model they implemented with SFH.
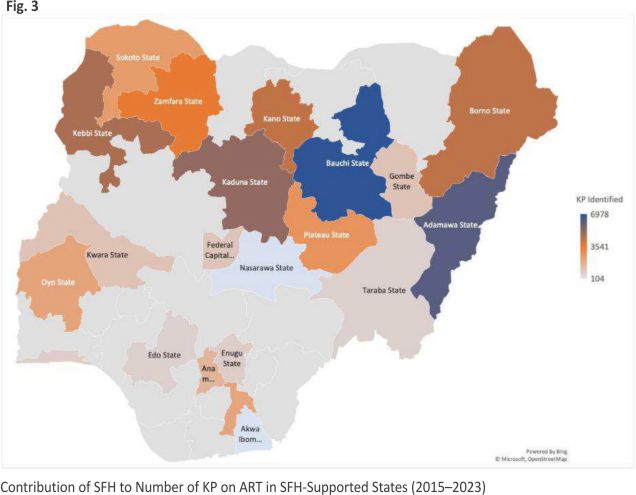
Overall, since it transitioned to a comprehensive HIV service partner, SFH has made significant contributions to Nigeria’s current efforts towards ending the HIV epidemic in 2030, to which reaching KPs with the HIV prevention and treatment services they need is central. SFH’s contribution to ART scale-up in each of its program states is shown in Fig. 3. On average, SFH contributed 95.5% to the KPs identified and placed on ART in each of its project states.
 SFH’s client-centered approach to programming, which resulted in the organization’s remarkable feats in promoting correct and consistent condom use, facilitated the OSS’s design and transition of existing ART health facilities to KP-friendly facilities in ways that promoted ownership and utilization by the KP community 39. Client-centered approaches to care, such as tailoring messages to particular client demography, and ensuring cultural appropriateness of strategies, help to create a safe, welcoming environment. This client-centered and community-oriented progra- mming, which includes close collaboration with state and non-state actors at various levels, helped the organization overcome some of its challenges. Some of these challenges included the reluctance of women to submit to available HTS due to persisting stigma, the preponderance of false addresses provided by clients, and security challenges. Lack of money to pay some user fees and for transportation to the facilities were some of the initial reasons for the reluctance of KPs to access services. Although our KP programs are designed to address these challenges, at a system level, the ability of countries to integrate HIV services into primary health care and into minimum service packages as part of efforts to attain Universal Health Coverage will go a long way to address these challenges 40. The UHC perspective on HIV programming could also help provide HIV services to under-represented/ marginalized populations, which is yet another persistent challenge in our program. In Nigeria, this means including HIV prevention and treatment services in the minimum service package under the Basic Health Care Provision Fund (BHCPF). This BHCPF is a health financing reform enacted under the National Health Act of 2014 to increase the coverage of quality basic health services and promote UHC in Nigeria. Through the BHCPF, poor Nigerians who are unable to pay health insurance premiums receive coverage for a set of minimum healthcare services. Although the fund now covers mostly reproductive, maternal, and child health services, there is scope for the fund to be expanded to cover HIV services for the poor. Initially funded from 1% of the country’s consolidated revenue fund, the Act establishing the fund provides for its expansion through special vehicles, such as sin and other pro-poor health taxes. There are also ongoing discussions and pressures from technocrats and civil society groups calling for increasing the primary source of the BHCPF from 1 to 2% of the CRF.
SFH’s client-centered approach to programming, which resulted in the organization’s remarkable feats in promoting correct and consistent condom use, facilitated the OSS’s design and transition of existing ART health facilities to KP-friendly facilities in ways that promoted ownership and utilization by the KP community 39. Client-centered approaches to care, such as tailoring messages to particular client demography, and ensuring cultural appropriateness of strategies, help to create a safe, welcoming environment. This client-centered and community-oriented progra- mming, which includes close collaboration with state and non-state actors at various levels, helped the organization overcome some of its challenges. Some of these challenges included the reluctance of women to submit to available HTS due to persisting stigma, the preponderance of false addresses provided by clients, and security challenges. Lack of money to pay some user fees and for transportation to the facilities were some of the initial reasons for the reluctance of KPs to access services. Although our KP programs are designed to address these challenges, at a system level, the ability of countries to integrate HIV services into primary health care and into minimum service packages as part of efforts to attain Universal Health Coverage will go a long way to address these challenges 40. The UHC perspective on HIV programming could also help provide HIV services to under-represented/ marginalized populations, which is yet another persistent challenge in our program. In Nigeria, this means including HIV prevention and treatment services in the minimum service package under the Basic Health Care Provision Fund (BHCPF). This BHCPF is a health financing reform enacted under the National Health Act of 2014 to increase the coverage of quality basic health services and promote UHC in Nigeria. Through the BHCPF, poor Nigerians who are unable to pay health insurance premiums receive coverage for a set of minimum healthcare services. Although the fund now covers mostly reproductive, maternal, and child health services, there is scope for the fund to be expanded to cover HIV services for the poor. Initially funded from 1% of the country’s consolidated revenue fund, the Act establishing the fund provides for its expansion through special vehicles, such as sin and other pro-poor health taxes. There are also ongoing discussions and pressures from technocrats and civil society groups calling for increasing the primary source of the BHCPF from 1 to 2% of the CRF.
This paper has some limitations. Instead of a narrative report approach, a life-course evaluation report, with structured baseline, mid-term, and end-term evaluation, would have provided a more in-depth, clear, and consistent track of SFH’s transformation over time and the outcomes achieved in the process. Linked to this limitation, is the lack of data on outcomes, which is affected, first, by the absence of an integrated evaluation of the transformation, and second, by the inability to attribute national outcome reports for the country’s HIV program to the work of specific partners, like the SFH. However, although largely output-based, program performance data provides valuable insight into programs’ contributions toward desired outcomes and impact. Thus, the details of SFH’s transformation from a prevention-only to a comprehensive prevention, treatment, and care program shared in this paper, including the program performance data may be useful for other organizations considering similar transitions.
Conclusion
The transition of SFH to a comprehensive HIV prevention, care, and treatment provider and its contributions to Nigeria’s efforts to scale up its treatment and other objectives toward attaining the UNAIDS 95-95-95 targets are lessons in growth, resilience, and a client-centered approach to care. They are also lessons on the enduring nature of community-engaged HIV programming, which UNAIDS acknowledges as the key to ending the HIV epidemic.
Despite nearly a decade in its transition and SFH’s contribution to increasing ART coverage in Nigeria, the need to scale up ART coverage for KPs is glaring. For sustainability, it is important for future scale-up efforts to be undertaken within a framework of PHC integration and UHC.
Data availability
No datasets were generated or analysed during the current study.
References
1. Salihu A, Jahun I, Oyedeji DO, Fajemisin W, Idogho O, Shehu S, Yakubu A, Anyanti J. Scaling up access to antiretroviral treatment for HIV: lessons from a key populations program in Nigeria. AIDS Res Therapy. 2025;22(1):10.
2. World Health Organization. HIV statistics, globally and by WHO region. 2023.
3. Onovo AA, Adeyemi A, Onime D, Kalnoky M, Kagniniwa B, Dessie M, et al. Estimation of HIV prevalence and burden in Nigeria: a Bayesian predictive modelling study. EclinicalMedicine.2023;62:10209 8.
4. United Nations Nigeria. From the darkest of days to a new dawn: 35 years of the Nigerian response to HIV and AIDS. Abuja: Joint United Nations Programme on HIV/AIDS; 2022.
5. UNAIDS. UNAIDS data 2022. Geneva: Joint United Nations Programme on HIV/AIDS; 2022.
6. Naiis. Nigeria HIV/AIDS indicator and impact survey. 2019.
7. Federal Ministry of Health. Integrated Biological & Behavioural Surveillance among Key Populations in Nigeria. Abuja: National AIDS & STI Control Program, FMOH; 2020.
8. Nigeria: Same Sex Marriage (Prohi- bition) Act, 2013. Refworld. Refworld —UNHCR’s Global Law and Policy Data base; 2023. https://www. refworld.org/legal/legislation/natlegbod/2013/en/19556.
9. Schwartz SR, Nowak RG, Orazulike I, Keshinro B, Ake J, Kennedy S, et al. The immediate effect of the Same-Sex Marriage Prohibition Act on stigma, discrimination, and engagement on HIV prevention and treatment services in men who have sex with men in Nigeria: analysis of prospective data from the TRUST cohort. Lancet HIV. 2015;2:e299-306.
10. Abah I, Tomescu S, Akpan F, Ondura E, Dauda SD. Assessing the care and treatment provided by USAID-supported key population projects in Nigeria. Washington: Data.FI, Palladium; 2022.
11. Lyons CE, Schwartz SR, Murray SM, Shannon K, Diouf D, Mothopeng T, et al. The role of sex work laws and stigmas in increasing HIV risks among sex workers. Nat Commun. 2020; 11:773.
12. Reeves A, Steele S, Stuckler D, McKee M, Amato-Gauci A, Semenza JC. National sex work policy and HIV prevalence among sex workers: an ecological regression analysis of 27 European countries. Lancet HIV. 2017;4:e134–40.
13. DeBeck K, Cheng T, Montaner JS, Beyrer C, Elliott R, Sherman S, et al. HIV and the criminalisation of drug use among people who inject drugs: a systematic review. Lancet HIV. 2017; 4:e357–74.
14. Patterson SE, Milloy M-J, Ogilvie G, Greene S, Nicholson V, Vonn M, et al. The impact of criminalization of HIV non-disclosure on the healthcare engagement of women living with HIV in Canada: a comprehensive review of the evidence. J Int AIDS Soc. 2015; 18:20572.
15. Shannon K, Strathdee SA, Goldenberg SM, Duff P, Mwangi P, Rusakova M, et al. Global epidemiology of HIV among female sex workers: influence of structural determinants. Lancet. 2015;385:55–7 1.
16. Gesesew HA, Tesfay Gebremedhin A, Demissie TD, Kerie MW, Sudhakar M, Mwanri L. Significant association between perceived HIV related stigma and late presentation for HIV/AIDS care in low and middle-income countries: a systematic review and meta-analysis. PLoS ONE. 2017;12: e0173928.
17. Nasidi A, Harry TO. The epidemiology of HIV in Nigeria. In: Adeyi O, Kanki PJ, Odutolu O, Idoko JA, editors. AIDS in Nigeria: a nation on the threshold. Cambridge: Harvard Center for Population and Development Studies; 2006.
18. Anyanti J, Ankomah A. An evaluation of a QuasiExperimental Community level HIV intervention in Nigeria. Soc Fam Health. 2005. https://doi. org/10.13140/RG.2.1.4185.0649.
19. Programme ENHR (enr). MARPs sensitization: a diversity training guide for health care providers in Nigeria. Population Council; 2012. https://knowledgecommons. popcouncil.org/departments_sbsr-hiv/320.
20. Society for Family Health. Expanded Social Marketing Project In Nigeria (ESMPIN) technical briefs. Abuja: Society for Family Health; 2016.
21. Awofala AA, Ogundele OE. HIV epidemiology in Nigeria. Saudi J Biol Sci. 2018;25:697–703.
22. Hassan AO, Oladeji AO, Osinowo K, Ajuwon AJ, Atibioke OP, Ojomo OA, et al. Effects of peer education on AIDS knowledge and sexual behavior among youths on national service and secondary school students in Nigeria. Int J Public Health Epidemiol. 2014;3:035–47.
23. UK-Foreign, Commonwealth Develop-ment Office. Enhancing Nigeria’s response to HIV and AIDS: Project completion review. FCDO; 2017. https://iati.fcdo.gov.uk/iati_ documents/5730662.odt.
24. Marseille E, Hofmann PB, Kahn JG. HIV prevention before HAART in sub-Saharan Africa. Lancet. 2002; 359:1851–6.
25. Entonu PE, Agwale SM. A review of the epidemiology, prevention and treatment of human immuno- deficiency virus infection in Nigeria. Braz J Infect Dis. 2007;11:579–90.
26. Idigbe EO, Adewole TA, Eisen G, Kanki P, Odunukwe NN, Onwujekwe DI, et al. Management of HIV-1 infection with a combination of nevirapine, stavudine, and lamivudine: a preliminary report on the Nigerian antiretroviral program. J Acquir Immune Defic Syndr. 2005;40:65–9.
27. Nigeria USM. PEPFAR: 20 years of impact. U.S. Embassy and Consulate in Nigeria. 2023. https://ng.usem- bassy.gov/pepfar-20-years-of-impact/.
28. Herrick B. Where is PEPFAR’s strategy for key populations?. Health Global Access Project; 2021.https:// healthgap.org/wp-content/ uploads/2021/09/PEPFAR-Key-Populations. pdf.
29. Abubakar Saleh J-E. Barriers to HIV/AIDS treatment in Nigeria. Am Indian Alsk Native Ment Health Res. 2015;3:305.
30. Ibiloye O, Jwanle P, Masquillier C, Van Belle S, Jaachi E, Amoo O, et al. Long-term retention and predictors of attrition for key populations receiving antiretroviral treatment through community-based ART in Benue State Nigeria: a retrospective cohort study. PLoS ONE. 2021;16: e0260557.
31. Azia IN, Mukumbang FC, van Wyk B. Barriers to adherence to antiretroviral treatment in a regional hospital in Vredenburg, Western Cape, South Africa. S Afr J HIV Med. 2016;17:476.
32. World Health Organization. Consoli- dated guidelines on HIV prevention, testing, treatment, service delivery and monitoring: recommendations for a public health approach. Genève: World Health Organization; 2021.
33. Aung NHHL, Soe KT, Kumar AMV, Saw S, Aung ST. What are the barriers for uptake of antiretroviral therapy in HIV-infected tuberculosis patients? A mixed-methods Study from Ayeyawady Region, Myanmar. Trop Med Infect Dis. 2020. https:// doi.org/10.3390/tropicalmed5010041.
34. Balogun A, Bissell P, Saddiq M. Negotiating access to the Nigerian healthcare system: the experiences of HIV-positive men who have sex with men. Cult Health Sex. 2020; 22:233 –46.
35. Arimoro AE. The criminalisation of consensual same-sex sexual conduct in nigeria: a critique. J Hum Rights Soc Work. 2019; 4:257–66.
36. World Health Organization. Consolidated guidelines on HIV, viral hepatitis and STI for key populations—2022. Geneva: World Health Organization; 2022.
37. Okonkwo P, Olatoregun OJ, Abolarin O, Olajide O. Barriers to accessing antiretroviral treatment among key populations in Southwest Nigeria. Cureus. 2024;16: e59312.
38. Duby Z, Nkosi B, Scheibe A, Brown B, Bekker L-G. “Scared of going to the clinic”: contextualising healthcare access for men who have sex with men, female sex workers and people who use drugs in two South African cities. S Afr J HIV Med. 2018;19:701.
39. NORC Walsh Center for Rural Health Analysis and University of Minnesota Rural Health Research Center. Rural HIV/AIDS Prevention and Treatment Toolkit. Rural Health Information Hub. Rural Health Information Hub; 2022. https://www.ruralhealth info.org /toolkits /hiv-aids.
40. Sparkes SP, Kutzin J. HIV prevention and care as part of universal health coverage. Bull World Health Organ. 2020;98: 80-80A.
Acknowledgements
The authors acknowledge the enormous contributions from USAID and GFATM for the grants awarded to SHF by these organizations to enable it to achieve its mission. All SFH’s partners that have contributed to the success achieved by SFH are profoundly appreciated.
Funding
This research has been supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) through the United State Agency for International Development (USAID) under the terms of USAID Cooperative Agreement No. 7206201900009. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the funding agencies.
Author information
Authors and Affiliations
Society for Family Health, Abuja, Nigeria
Abdulsamad Salihu, David Olusegun Oyedeji, Wole Fajemisin, Omokhudu Idogho, Samira Shehu & Jennifer Anyanti
Rady Faculty of Health Sciences, University of Manitoba, Winnipeg, Canada
Ibrahim Jahun
Center for Bioethics and Research, Ibadan, Nigeria
Aminu Yakubu
Federal Ministry of Health, Abuja, Nigeria
Aminu Yakubu
Contributions
A.S and I.J conceptualize and wrote the manuscript D.O and W.F. conduct design and analysis O.I, S.S. and Y.A. drafted the work substantially and interpreted data J.A. provided overall leadership, conceptualize and drafted the work substantially.
Corresponding author
Correspondence to Ibrahim Jahun.
Ethics declarations
Competing interests
The authors declare no competing interests.
Credit: Salihu, A., Jahun, I., Oyedeji, D.O. et al. Correction to: Scaling up access to antiretroviral treatment for HIV: lessons from a key populations program in Nigeria. AIDS Res Ther 22, 23 (2025). https://doi.org/ 10.1186/s12981-025-00722-y
: an evolving threat to the Nigerian health system – a review")



: an evolving threat to the Nigerian health system – a review")

