

Judith I Ukwajiunor, Okwuoma C Abanobi, Chikere Ifeanyi C Ebirim*, Sally NO Ibe and Christain C Nwachukwu Department of Public Health, Federal University of Technology, Owerri, Nigeria *Corresponding Author: Owerri, Nigeria, PMB 1526, Owerri, Nigeria, Tel: 08038870206, 08123293306 E-mail: chayke2000@yahoo.com Chikere Ifeanyi C Ebirim, Department of Public Health, Federal University of Technology,
[mks_button size=”small” title=”Download the PDF” style=”squared” url=”https://clinicalhealthjournal.com/wp-content/uploads/2020/10/Risk-Factors-of-Sexually-Transmitted-Infections-among.pdf” target=”_self” bg_color=”#000000″ txt_color=”#FFFFFF” icon=”” icon_type=”” nofollow=”0″]
Abstract
Background: Sexually Transmitted Infections (STIs) are a major public health concern which is responsible for acute illness, infertility, long-term disability and death globally. The adverse effect is however profound in developing countries and among women when left untreated. In Nigeria, the Boko haram insurgence and other conflicts has given rise to internally displaced persons. The increased reports of STIs among internally displaced persons which women and children make up the largest population and the dearth of literature on epidemiological studies on STIs among internally displaced persons initiated the need for the study.
Aim: This study seeks to determine the risk factors of Sexually Transmitted Infections (STIs) among internally displaced women of child bearing age in Internally Displaced Persons Camps in Abuja.
Methodology: A community based retrospective case-control study design was used. Each consenting participant was screened to detect the presence of antibodies for Hepatitis B, C, HIV, and Syphilis using Rapid Diagnostic Tests. A self- administered structured questionnaire was used to assess risk factors among study participants after being validated and its reliability tested. Multistage sampling technique was used to select the study participants (n=362) and Cases and Controls were selected using set criteria.
Results: Data was entered and analysed using SPSS version 21. Chi- square was used to determine the association between variables and STI morbidity within the period of 6months and above prior to the study. Variables found to be significant in the analysis were entered into a multivariate logistic regression model to estimate the strength of the associations between these variables and STI morbidity. P-value<0.05 was considered statistically significant. With respects to Influence of socio-demographic characteristics as a risk-factor of STI there was significant association between marital status and STI morbidity. (X2=8.445, P=0.004).
Sexual behaviours which were significantly associated as risk-factors of STIs were number of sexual partners (X2=4.032, P=0.045), use of sexual performance enhancers (X2= 12.302, P=0.001). Furthermore, getting a reward for sex a variable of gender-based violence had a very significant association with STIs morbidity (X2= 7.086, P=0.008). IDP mobility as a risk-factor for STI revealed that the nature of relationships study participants had outside the IDP camp was significantly associated with STIs (X2=5.710, P=0. 017). The adjusted logistic regression model showed that the likelihood of STI morbidity was 1.8 times more among single respondents when compared to married respondents (OR=1.8). Respondents with no sexual partners were 1.5 times more likely to get an STI when compared with those who had sexual partners (OR=1.5). Furthermore, respondents who used sexual performance enhancers were 2.9 times more likely to have an STI when compared with those who used no form of sexual performance enhancer (OR=2.923, P-value=0.001).
Conclusion: This study found that risk factors for STIs which exists among internally displaced women of child bearing age in IDP camps in Abuja were; marital status, having a sexual partner, getting a reward for sex and having sexual relationships outside the IDP camp. However, the logistic regression model revealed that the use of sexual performance enhancers (OR=2.923 P=0.001 95% CI [1.597–5.348]) was the most significant risk factor of STIs among the study group. Thus, there is need for more comprehensive community based STI studies alongside implementation of risk targeted Public health intervention. Keywords: STIs; Risk factors; IDPs.
Introduction:
Over 1 million cases of Sexually Transmitted Infections (STIs) are recorded daily
 worldwide with a global estimate of 357 million new infections of STIs occurring 1 yearly . In most developing countries, STIs and their complications are among the top five diseases for which sexually active adults seek health care. According to WHO, women of childbearing age which are women within the ages of 15-49 years bear the brunt of major complications resulting from STIs such as infertility, chronic pelvic pain, pelvic inflammatory diseases and ectopic pregnancy.
worldwide with a global estimate of 357 million new infections of STIs occurring 1 yearly . In most developing countries, STIs and their complications are among the top five diseases for which sexually active adults seek health care. According to WHO, women of childbearing age which are women within the ages of 15-49 years bear the brunt of major complications resulting from STIs such as infertility, chronic pelvic pain, pelvic inflammatory diseases and ectopic pregnancy.
This is because as research has shown most women with STIs are entirely asymptomatic, pauci-symptomatic and even when symptoms exist, they are often unrecognized. Thus, many women do not seek timely treatment for STIs which has led to severe underreporting and underestimation of the true incidence and aetiology of STIs in women.
In Africa, 12.4 million persons have been displaced as a result of conflict and war; this is about 30 percent of the total number of people internally displaced by 2 conflict globally . Nigeria has 3.3 million Internally Displaced Persons (IDPs), the largest in Sub-Saharan Africa and the third largest globally with about 90 per cent 3 attributed to fleeing from Boko Haram insurgence . This insurgence has led to the displacement of persons from their homes into forced migration. This situation has led to the formation of temporary, informal settlements and integrated settlements among host communities as IDP locations within the FCT and other States.

There are about 20,659 Internally Displaced Persons (IDPs) in FCT originating mainly 4 from Borno, Yobe and Adamawa States . 22 percent of these IDPs reside in official IDP camps and camP-like settings, while the majority reside within the host community. The Nigerian National Population Commission estimates that 80 percent of IDPs in Nigeria are women and children.
The decreased number of males was attributed mainly to their deaths during violence eruptions as they usually tend to protect and defend their families. More so, rescue of women and children taken as captives by the Boko Haram is more prevalent than that of men, hence, their increased population among the displaced persons. Furthermore, religious practices of early marriage and polygamy which is common among people from Borno, Adamawa and Yobe states encourages an increase in the population of women of child- bearing age as against their male counterpart.
Widowed women and orphaned female children who have been displaced are the most vulnerable group easily exposed to series of protection risks which maybe drivers of sexual risk behaviours such as sexual violence, transactional sex for food and other basic amenities. Some media reports have alleged camp officials who are supposedly in charge of the IDPs, security personnel and even members of the community in cases where IDPs are in integrated communities of 5 rape, sexual harassment and even gender based violence . This in itself is a silent killer as affected women may not report due to shame and fear and they may be infected with STIs. Furthermore, the dearth of data on STIs in IDP camps in Nigeria and risk factors causally related to the STIs have prompted this study.
Methodology:
A community-based, retrospective case- control study design and multistage sampling method was used for the study. This research design was chosen because the study population share common properties of being internally displaced and resident within a confined space called an IDP camp. Also, the study intends to compare respondents who have the highlighted disease or outcome (cases) with patients who do not have the disease or outcome (controls), and look back retrospectively with the aid of a questionnaire to compare how frequently the exposure to a risk factor is present in each group so as to determine the relationship between risk factor and the disease. Thus, the study is designed to not only measure association but also calculate odds ratio which is a measure of association that quantifies the relationship between an exposure and two categories of health outcome.
Cases were defined as any internally displaced woman within the ages 15-49 years resident in the IDP camp for six months and above prior to the study period who may or may not show symptoms of STIs and is confirmed positive of any of the STI under study (HIV/AIDS, Hepatitis B, Hepatitis C and syphilis) either via laboratory tests or screening. Controls were defined as any internally displaced woman within the ages 15-49 years resident in the IDP camp for the past six months and above prior to the study period who has no symptoms of STIs and is confirmed negative of HIV/AIDS, Hepatitis B, C and Syphilis via laboratory diagnosis or screening.
The controls were derived from the population of non- cases. Matching of cases to controls was based on the following confounding characteristics; age, marital status, sexual behaviour and duration of residence in IDP camps. Matching of cases and control was done using frequency matching method.
Inclusion criteria
Any internally displaced woman of child-bearing- age between the ages of 15-49 who has been resident in the IDP camp for at least 6months and above and not currently receiving treatment for any STI. In addition, to participate in the study the woman must give informed consent.
Exclusion criteria
Women of child bearing age who are not internally displaced although resident in the camp. Women who are already on Antiretroviral Therapy (ART) and who do not give their informed consent were excluded from this study.
Serologically, data was collected using the following instruments: alcohol swab, sterile specimen collection bottle, tourniquet, syringe and Rapid Test Kits for antibody test for Hepatitis B, C, HIV and Syphilis. Also, a self-administered questionnaire with four sections namely; socio-demographic characteristics, sexual behaviour, prior exposure to gender-based violence and IDPs mobility was used to collect information on risk factors exposure.
A written informed consent was obtained from each respondent before data was collected and the Federal Capital Territory Health Research Ethics committee gave Ethical approval for the research with research number (FHREC/2018/01/122/29-10-18). The data was analyzed using Statistical Package for Social Science (SPSS) version 21.0 computer software and the results were presented in simple frequency and percentages.
Sample size
The population of women of child- bearing age in IDPs in Abuja are estimated to 4 be about 11,155 which are 54 percent of the total number of IDPs 20,659 . The sample size was obtained using the sample size formula for case control study (Appendix A) and the sample size calculated was 362 respondents. In the multistage sampling method used for this study, the following steps were carried out: ? Abuja Municipal Area Council was categorised into wards which were twelve in number namely; City centre, Garki, Kabusa, Wuse, Gwarimpa, Jiwa, Gui, Karshi, Orozo, Karu, Nyanya and Gwagwa. The number of IDP camps in each ward was then indicated (Appendix B). ? Wards which have IDP camps were then purposively selected for the study. There were nine IDP camps in AMAC. The IDP camps were further classified (stratified) into types namely; integrated and non-integrated camps (Appendix C).
There were two integrated camps and seven non- integrated camps. ? Using the list of IDP camps simple random sampling by balloting without replacement was carried out proportionately for each type of camp. Using onethird proportion, one camp was selected from the integrated camps and two camps from the non-integrated camps. ? The population of women of child-bearing age in each selected IDP camp was then established. The study sample was gotten using simple random sampling technique. In each of the IDP camps selected, displaced women of child -bearing age were classified as cases or non-cases with the aid of the case definition. Controls were later selected from the non-cases and matched frequency-wise using adequate variables. Copies of the questionnaire were then administered to cases and controls to find out exposure variables.
Results
Influence of socio-demographic characteristics as a risk-factor of ST
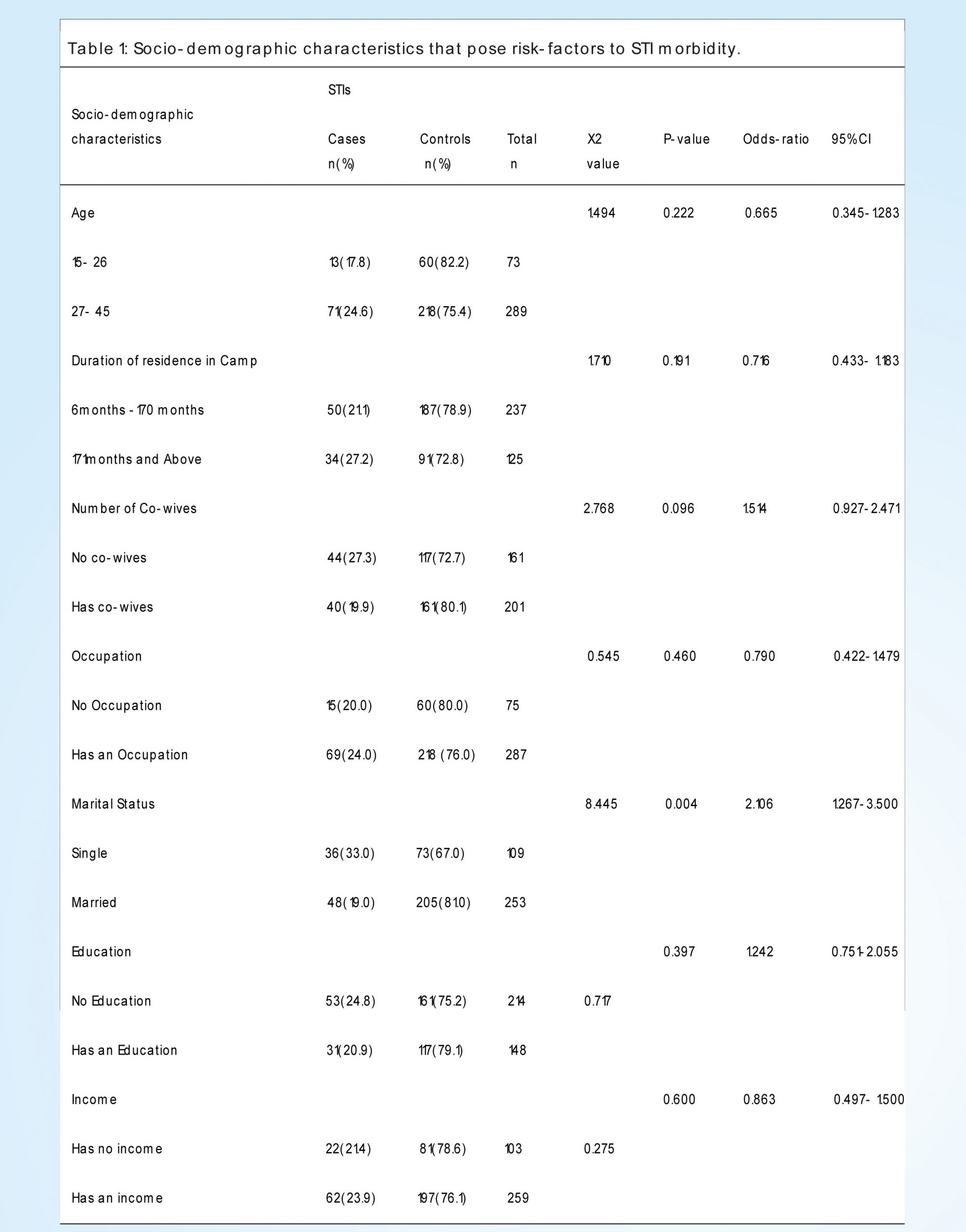
In Table 1, the socio-demographic factors that pose as risk-factors for STIs are documented. It indicated that of the 73 respondents aged 15-26 years, 60(82.2%) were negative for STI whereas 13(17.8%) reported testing positive for STI. Among the respondents aged 27-45, 218(75.4%) were negative while 71(24.6%) were positive for STIs.
The odds ratio show that age has a 0.7 likelihood to influence STI morbidity. The result also shows a non- significant statistical association between age and STI occurrence. (X2=1.494, P=0.222 OR= 0.665, 95% CI=0.345- 1.283). The table also presents 237 respondents who had resided in the IDP camp for the period of 6-170 months, 187(78. 9%) were negative to STI while 50(21.1) were positive to STI.
Also, of the 125 respondents who had resided for about 171months and above in the camp, 91(72.8%) indicated that they were negative to STI while 34(27.2%) were positive. The likelihood of being STI positive was 0.716 times more among cases exposed to duration of residence in IDP camp when compared to cases This result shows that there is no significant relationship between duration of residence at camp and STI occurrence. Furthermore, the duration of residence in the IDP camp had a 0.7 likelihood to influence STI morbidity. (X2=1.710, P=0.191 OR=0.716, 95% CI=0.433-1.183).
Of the 161 respondents who stated that they had no co-wives, 117(72.7%) tested negative to STIs while 44(27.3%) were positive to STIs. Also, of the 201 respondents that said they had co-wives, 161(80.1%) tested negative to STIs while 40(19.9%) tested negative to STIs. The number of co-wives had a 1.5 times odds to influence STI morbidity. The result also showed no significant association between number of co-wives and STI morbidity (X2=2.768, P=0.096 OR=1.514, 95%CI=0.927-2.471). The result shows that of the 75 respondents who had no occupation, 60(80.0%) had negative STIs results whereas 15(20.0%) had positive STIs results. Of the 287 respondents who had an occupation, 218(76.0%) had negative STI results while 69(24.0%) had positive STI result. Occupation had a 0.8 likelihood to influence STI morbidity. In addition, the result showed that there is no significant association between occupation and STI morbidity (X2= 0.545, P=0.460 OR=0.790, 95%CI = 0.422-1.479).
Based on the results on the table, 109 respondents were single of which 73(67.0%) were STI negative and 36(33. 0%) were STI positive. Furthermore, 253 respondents were married of this group, 205(81.0%) tested negative to STI while 48(19.0%) tested positive to STI. Marital status had a 2 times likelihood to influence getting an STI. Thus, the result showed that there is significant association between marital status and STI morbidity (X2=8.445, P=0.004 OR=2.106, 95%CI=1.267– 3.500).
The results also revealed that of the 214 respondents that have no education, 161(75.2%) tested negative to STI while 53(24.8%) tested positive to STI. Of the 148 respondents that have an education, 117(79.1%) did not have an STI while 31(20.9%) had an STI. The educational qualification of a respondent was seen to have a 1.2 times odds of STI morbidity. In addition, the result showed that there is no significant association between education and STI morbidity (X2=0.717, P=0.397 OR=1.242, 95% CI=0.751-2.055). The table also presents that of the 103 respondents that had no income, 81(78.6%) had no STI while 22(21.4%) were positive for an STI. Of the 259 respondents, 197(76.1%) had no STI and the other 62(23.9%) had an STI. The odds of STI morbidity based on influence of income was 0.9. In addition, the results showed no significant association between income and STI morbidity (X2=0.275, P=0.600 OR=0.863, CI=0.497- 1.500).
Influence of sexual behaviours as a risk-factor of STIs
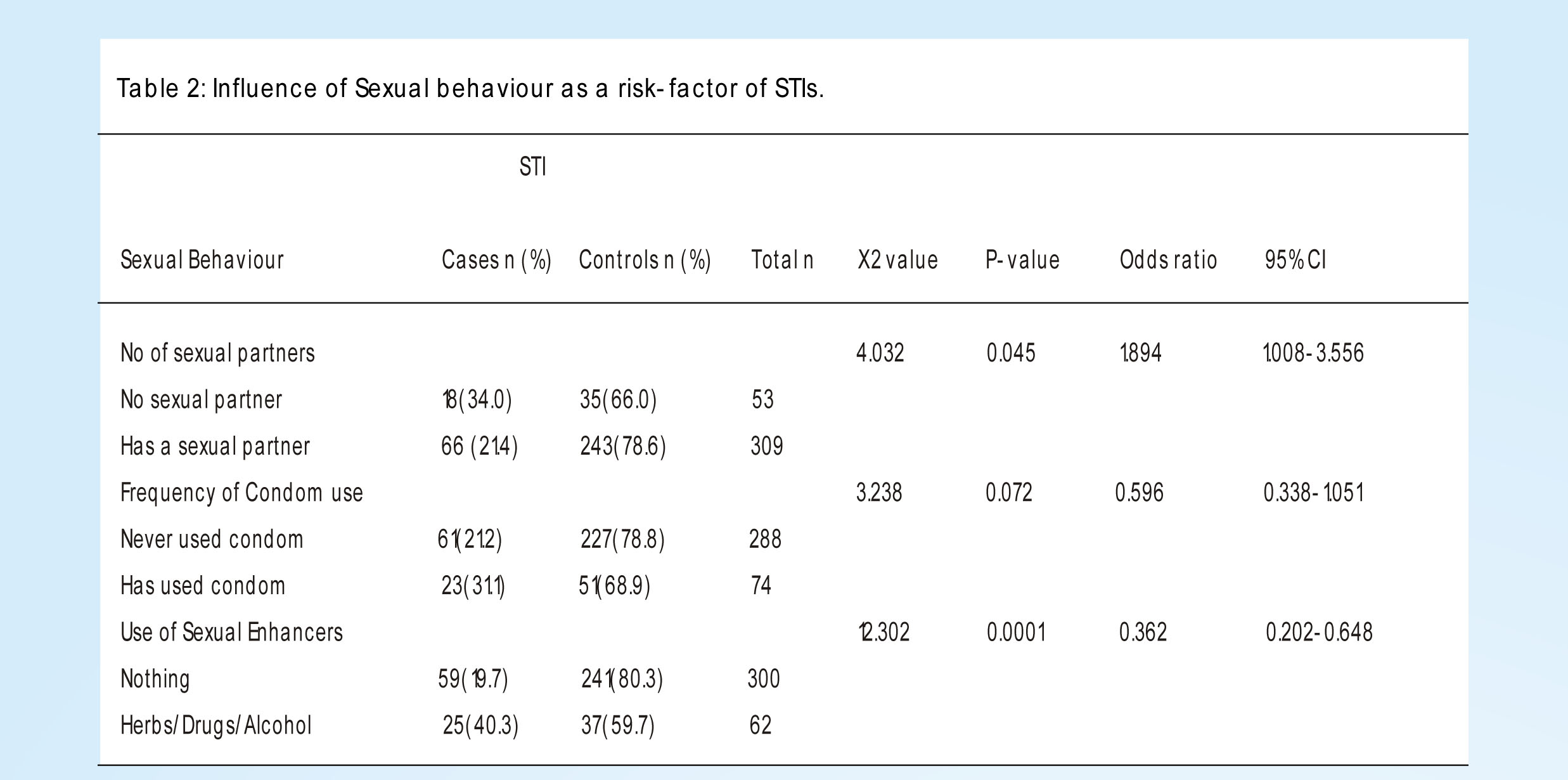
In Table 2, the sexual behaviours that are risk factors of STIs were documented. It indicated that of the 53 respondents who had no sexual partners, 35(66.0%) tested negative for STI and 18(34.0%) were positive. Of the 309 respondents who have had a sexual partner, 243(78.6%) were tested negative for STI whereas 66(21.4%) tested positive for STI. The number of sexual partner had a 1.9 times likelihood to influence STI among study group. The results thus showed a significant association between no of sexual partners and STI morbidity. (X2=4. 032, P=0.045 OR=1.894, CI=0.497-1.500) Documented on the table is the frequency of condom use. Of the 288 respondents who have never used condom, 227(78.8%) do not have STI while 61(21.2%) have an STI. For the group of respondents who had used condom, 51(68.9%) did not have STI while 23(31.1%) tested positive to STI. Condom use had a 0.6 likelihood to influence STI. In addition, the results shows that there is no significant relationship between frequency of condom use and STIs. (X2=3.328, P=0.072, OR=0.596, CI=0.338-1.051). Also, indicated on the table is the use of sexual enhancers by respondent. Of the 300 respondents who used nothing for sexual enhancement, 241(80.3%) were STI negative and the 59(19.7%) respondents tested positive for STI. 62 respondents indicated the use of herbs /drugs/Alcohol as sexual performance enhancers. 37(59.7%) respondents tested negative for STI while 25(40.3%) tested positive for STI. The use of sexual performance enhancers showed a 0.4 likelihood to influence STI morbidity. In addition, the results revealed that there is a significant relationship between use of sexual enhancers and STI morbidity. (X2=12.302, P=0.001 OR=0.362, CI=0.202 -0.648).
Influence of gender-based violence as a risk-factor for STI
In Table 3, prior exposure to gender based violence by respondents was recorded. It indicated that of the 309 respondents who had never been exposed to GBV, 241(78.0%) were negative to STI while 68(22.0%) were positive for STI. Among the group who had prior experience of GBV, 37(71.2%) were STI negative whereas 15(28.8%) were STI positive. Prior exposure to gender based violence had a 0.7 likelihood to influence STI morbidity. The table further showed that prior exposure to GBV has no significant relationship with STI morbidity (X2=1.176, P=0.278 OR=0.696, [95%CI=0.361- 1.343]).
The Table also presents that of the 300 respondents who received nothing as reward for sex 239(79.7%) were negative for STI and 61 (20.3%) were positive for STI. In the category of respondents who accepted food, job or money as reward for sex, 39(63.9%) respondents were STI negative and 22(36.1%) STI positive. Reward for sex had a 0.5 likelihood to influence STI morbidity among respondents. In addition the results revealed that there is a significant association between reward for sex and STI (X2=7.086, P=0.008 OR=0.452, [95%CI=0.250- 0.819]).
Table 3 describes the influence of IDP mobility as a risk-factor for STI. The results show that 344 respondents indicated free movement was practiced in the IDP camps. 264(76.7%) of the above number of respondents tested negative to STI while 80(23.3%) tested positive to STI. Of the 18 respondents who reported restricted movement in the IDP camps, 14(77.8) were STI negative and 4 (22.2%) were STI positive. This result showed that there is no significant association between IDP mobility and STIs. Also, IDP mobility had a 1.1 likelihood to influence STI morbidity (X2=1.000, P=0.591 OR=1.061, [95%CI= 0.340-3.313]).
The nature of relationships respondents have outside the IDP camp was also captured on the Table 4 respondents said they had non sexual relationships outside the camp and of this number, 254(78.6%) were STI negative whereas, 62(21.4%) respondents were STI positive. For the group that indicated that they had sexual relationships outside the camp, 24(61.5%) were tested negative of STIs with 15(38.5%) tested positive. This result further showed that there is a significant association between nature of relationship outside the camp and STIs. The nature of relationships respondents had outside the IDP camps had a 0.4 odds to influence STI morbidity (X2= 5.710, P= 0.017 OR=0.435, [95%CI= 0.216- 0.873]).
Multivariate logistic regression of risk-factors of STIs
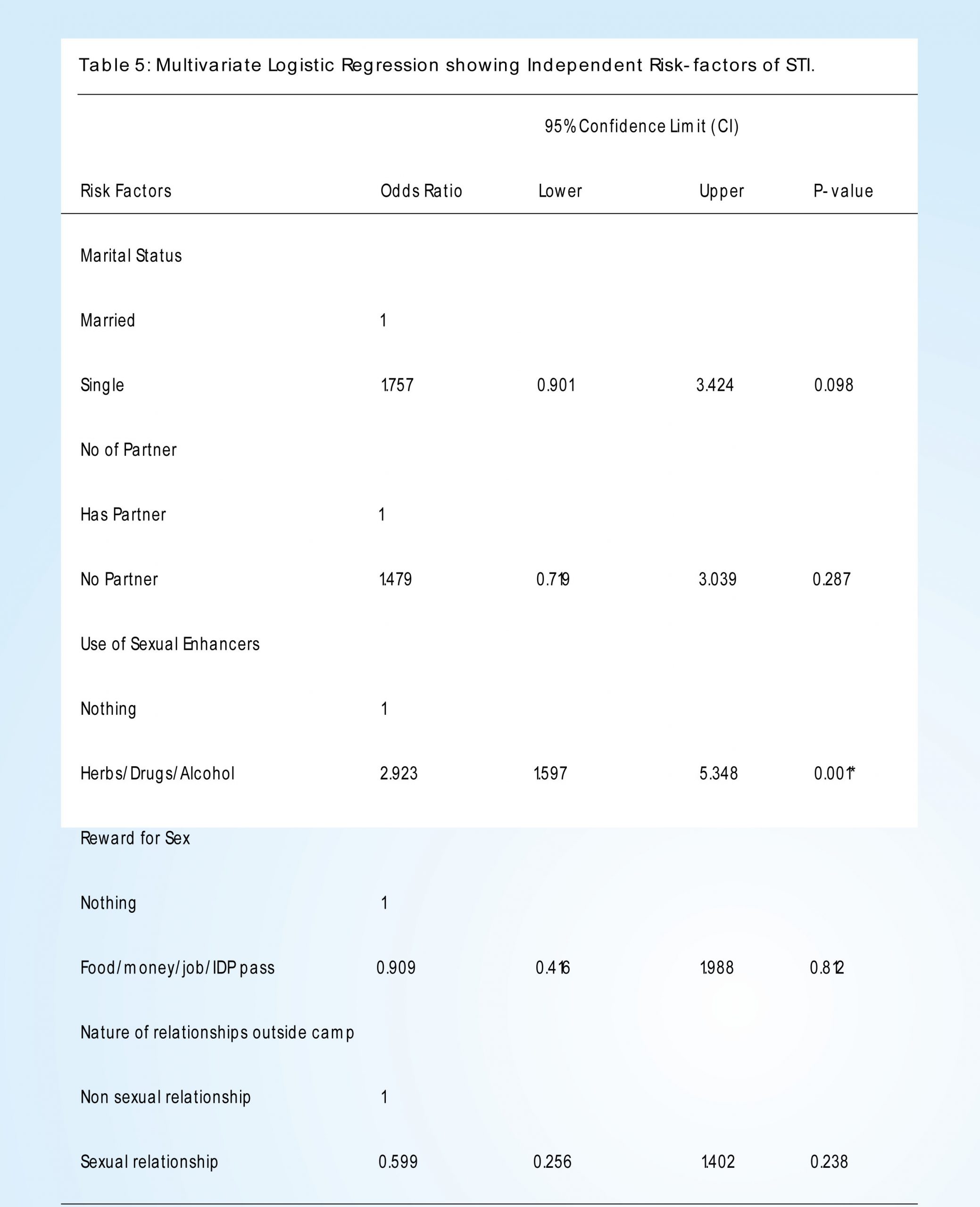
Table 5 below shows the adjusted logistic regression model using only significant independent risk factors of STIs. The logistic regression model showed that the likelihood of STI morbidity was 1.8 times more among single respondents when compared to married respondents (OR=1.757, P-value=0.098). Respondents with no sexual partners were 1.5 times more likely to get an STI when compared with those who had sexual partners (OR=1.479, P-value=0.287). Also, it was noted that the likelihood of STI morbidity was 0.6 times more among respondents with sexual relationships outside the IDP camps when compared with those who had nonsexual relationship outside the camps(OR=0.599, P-value=0.238). Respondents who received a reward for sex were 0.9 times more likely to get an STI when compared with those who received no form of reward for sex (OR=0.909, Pvalue=0.812).
Furthermore, respondents who used sexual performance enhancers were 2.9 times more likely to have an STI when compared with those who used no form of sexual performance enhancer (OR=2.923, P-value=0.001). Although the above risk factors showed significant association using Chi- square tool, in the logistic regression model only the use of sexual performance enhancers was seen to be statistically significant. Thus, the model shows that use of sexual performance is a true predictor of STI among internally displaced women of child bearing age resident in IDP camps. It indicates that use of sexual performance enhancers such as Alcohol, drugs and herbal mixtures is a major risk factor for STI among internally displaced women of child- bearing age as it was significantly associated to STI morbidity (OR=2.923, P-value=0.001). Respondents who are STI positive have 2.9 times the odds of using sexual enhancers than those who are STI negative.
Discussion
Major findings in this study from a total population of 362 persons were that the age group of 27-38 years had the largest population 148(40.9%) in the IDPs camp. Also, more internally displaced women 237(65.5%) have been resident in the IDP camp for 6-170 months. Majority of the women 206(56.9%) had never done an STI test before and were doing it for the first time thus unaware of their STI status previously. Also, 231(63.8%) a greater proportion of the internally displaced women are traders albeit petty traders. Furthermore, 214(59.1%), had no formal education and majority of the internally displaced women do not use condoms 284(78.5%) this may be due to male refusal to use, non- availability of condom.
When socio-demographic characteristics were considered in this study, result showed being single as a risk factor for STIs was significantly associated with STI 6morbidity. Previous studies by , which stated that being married (OR=0.4, 95% CI: 0.3–0.7) is inversely associated with STIs and [7], which stated that being single is directly associated with STIs [Odds Ratio (OR) 1.82, (95% CI 1.08, 3.05)] supported this finding. The reason for this may be because single persons are more likely to have multiple sexual relationships than married persons. However, the study by Maina is in contrast with this finding as it states that married participants were associated with higher infection rate (91%) than single participants (3.03%) this maybe because the respondents were drawn from STI clinics unlike this study which was community based.
Also, occupational status, age, duration of residence in IDPs camp and number of co-wives was not associated to STIs in this study. This corresponded with the 8findings by , in their study that there was no significant difference in age, and employment status between cases and controls. However, in other studies by, 6 9Ginindza, et al., , Saroj, Murthy, Kumar, & Kumar, , risk factors significantly associated with STIs were age and employment status (OR=0.9, 95% CI: 0.8-0.9), [Chi-square=7.669 and P-value=0.022] respectively .This difference in findings maybe as a result of the scope of this study which focused on only women unlike other studies which had men as part of their study population.
In previous studies by , there was significant association observed between per capita income and study groups [Chi-square=8.997, P-value=0.012] however, in this study income was not significantly associated to study groups this may be because income was calculated on monthly basis and not per capita and also the presence of male respondents in other studies.
With regards to sexual behaviour, this study noted that the number of sexual partners, and use of sexual enhancers were very significant for the STIs under study. The proportion of cases that used sexual enhancers compared with cases who did not was 40.3% to 19.7%. This findings corresponds with studies carried out 6 10 11by Ginindza, et al., , Men´endez et al., , Hughes, et al., , where risk factors for STI which were significant were alcohol consumption and having more than one sexual partner, having the partner living in another area, number of sexual partners and ever injected drugs respectively. In addition, studies by Saroj, 9Murthy, Kumar, & Kumar , which stated that a significantly higher proportion of cases liked to take alcohol/illicit drugs while having sex (46/106, 43.4% cases vs. 6/45, 13.3% controls, P<0.001) with an Odds ratio of 17.538 for those who had a 7history of alcohol intake supported this study findings. Basera, et al., , in their study reported Alcohol use influenced STI morbidity (OR 1.50, 95% CI 1.04, 2.16) and this concurred with this study.
With respects to behavioural factors, frequency of condom use which is a behavioural factor in this study was not statistically significant to STI. The study by 12Park, Seo, Jeong, & Lee , was in concurrence with this study as it reported that there was no significant difference between STIs and behavioural factors or sexual practices.
When Prior exposure to gender based violence was examined as a risk factor for STIs, this study showed that among cases of STIs, 28.8% had been victims of GBV at least once compared to 22.0% cases who had never experienced GBV. However, GBV was not significantly associated to STIs this did not matched previous studies 7by Basera, et al., , in which Prior exposure to gender based violence or sexual assault (OR 2.25, 95% CI 1.39, 3.63). This may be as a result of the difference in sample size as 362 respondents were used in this study compared to 3953 respondents of previous study.
Also, getting a reward for sex was noted as having a very significant association 13with STIs. This corresponded with studies by Adeniyi, et al., , where the odds of HIV infection were 1.4 times higher among women who had recently had transactional sex (adjusted OR 1.4, 95% CI 1.1–2.0) compared with others. Also, the 8study by Raj, et al., , concurred with this study because there was a higher proportion of cases that had sex in exchange for money or gift (52/106, 49% cases vs 4/45, 8.9% controls, P < 0.001) However, more cases (76.9%, 40 of 52 cases who had transactional sex, vs 50%, 2/4 controls) used condom while engaging in transactional sex, thus making the difference between the two groups not statistically significant (P=0.231). This further explains the effect of confounding variables in previous studies which was dealt with in present study using frequency matching.
9Based on existing literature , significant association was observed between history of migration and study groups. [Chi-square=9.617, P-value= 0.003]. Odds ratio between the STI/STD status and who had history of migration was 3.087 this was in concurrence with this study which showed that IDP mobility had a likelihood to influence STI.
Conclusion
Summarily, this study found that a significant number of risk factors exist among internally displaced women of child bearing age in IDP camps in Abuja. They include; being single, on monthly basis and not per capita and also the presence of male respondents in other studies.
With regards to sexual behaviour, this study noted that the number of sexual partners, and use of sexual enhancers were very significant for the STIs under study. The proportion of cases that used sexual enhancers compared with cases who did not was 40.3% to 19.7%. This findings corresponds with studies carried out 6 10 11by Ginindza, et al., , Men´endez et al., , Hughes, et al., , where risk factors for STI which were significant were alcohol consumption and having more than one sexual partner, having the partner living in another area, number of sexual partners and ever injected drugs respectively. In addition, studies by Saroj, 9Murthy, Kumar, & Kumar , which stated that a significantly higher proportion of cases liked to take alcohol/illicit drugs while having sex (46/106, 43.4% cases vs. 6/45, 13.3% controls, P<0.001) with an Odds ratio of 17.538 for those who had a 7history of alcohol intake supported this study findings. Basera, et al., , in their study reported Alcohol use influenced STI morbidity (OR 1.50, 95% CI 1.04, 2.16) and this concurred with this study.
With respects to behavioural factors, frequency of condom use which is a behavioural factor in this study was not statistically significant to STI. The study by 12Park, Seo, Jeong, & Lee , was in concurrence with this study as it reported that there was no significant difference between STIs and behavioural factors or sexual practices.
When Prior exposure to gender based violence was examined as a risk factor for STIs, this study showed that among cases of STIs, 28.8% had been victims of GBV at least once compared to 22.0% cases who had never experienced GBV. However, GBV was not significantly associated to STIs this did not matched previous studies 7by Basera, et al., , in which Prior exposure to gender based violence or sexual assault (OR 2.25, 95% CI 1.39, 3.63). This may be as a result of the difference in sample size as 362 respondents were used in this study compared to 3953 respondents of previous study.
Also, getting a reward for sex was noted as having a very significant association 13with STIs. This corresponded with studies by Adeniyi, et al., , where the odds of HIV infection were 1.4 times higher among women who had recently had transactional sex (adjusted OR 1.4, 95% CI 1.1–2.0) compared with others. Also, the 8study by Raj, et al., , concurred with this study because there was a higher proportion of cases that had sex in exchange for money or gift (52/106, 49% cases vs 4/45, 8.9% controls, P < 0.001) However, more cases (76.9%, 40 of 52 cases who had transactional sex, vs 50%, 2/4 controls) used condom while engaging in transactional sex, thus making the difference between the two groups not statistically significant (P=0.231). This further explains the effect of confounding variables in previous studies which was dealt with in present study using frequency matching.
Based on existing literature , significant association was observed between history of migration and study groups. [Chi-square=9.617, P-value= 0.003]. Odds ratio between the STI/STD status and who had history of migration was 3.087 this was in concurrence with this study which showed that IDP mobility had a likelihood to influence STI
Conclusion
Summarily, this study found that a significant number of risk factors exist among internally displaced women of child bearing age in IDP camps in Abuja. They include; being single, having a sexual partner, getting a reward for sex and having sexual relationships outside the IDP camp. When risk factors were considered based on the set objectives, marital status and age were major risk-factors identified under socio-demographic factors. For sexual behaviours; number of sexual partners, frequency of condom use and use of sexual performance enhancers were identified as risk factors for STIs in this study. When prior exposure to gender-based violence was measured, reward for sex was a significant risk factor for STI. IDP mobility revealed that the nature of relationship IDPs had outside the camp was a major predictor of STI.
Furthermore, the logistic regression model revealed that the use of sexual performance enhancers such as Alcohol, herbs and drugs to be the most significant risk factor STI.
Recommendations
After the conclusion of this study, the researcher made the following recommendations:
- Further studies can be carried out to identify peculiar risk factors of STIs among male IDPs
- Risk targeted public health intervention should be carried out systematically among IDPs so as to improve knowledge, awareness and prevention of STIs via mitigation of its risk factors.
- Sexual health programs should be implemented with the inclusion of gender sensitive and youth friendly centres within IDP camps so as to encourage health seeking behaviours.
- Routine screening should also be carried out among IDPs and treatment administered to confirmed cases of STI.
Acknowledgements
Special thanks to the FCT Health Research and Ethics Committee for giving me the opportunity to carry out this study, the Abuja Municipal Area Council (AMAC) Health Department, the IDP Camp Commandant (Mr. Mustapha Mohammed) and Heads of various IDP camps visited alongside the respondents for their support and collaboration towards the success of this work. Also my sincere gratitude to the former Director (Dr. H.N. Okoroukwu), the laboratory staff (Mrs. Abiola Ojo, Geraldine Odirichukwu, Mr. Egbe Friday, Ms. Eromo A.) and phlebotomists of the Department of Public Health, Abuja for their technical aid during the screening tests. Also, appreciation to the HIV/AIDS and STI control programme unit of the Department of Public Health for the HIV/AIDS test kits. Deepest thanks to Mr. & Mrs. J.U Ukwajiunor for funding this research and their undying support.
Authors’ contributions
Ukwajiunor Judith I. conceived the study, designed the instrument for data collection, performed data collection and manuscript drafting. Abanobi O.C, supervised the study and also contributed in study design, face validity of instrument of data collection and in-depth manuscript review. Ebirim C.I.C. performed the statistical analysis with interpretations and manuscript review. Ibe S.N.O. was responsible for giving content validity to the instrument for data collection and participated in review of related literature and critical review of the manuscript. Nwachukwu Christain C. aided with data collection and review of manuscript.
References
- Newman L, Rowley J, Vander Hoorn S, Wijesooriya NS, Unemo M, et al. (2015) Global estimates of the prevalence and incidence of four curable sexually transmitted infections in 2012 based on systematic review and global reporting. PLoS One 10: e0143304. Link: http://bit.ly/36I6ZVi
- Internal Displacement Monitoring Centre (IDMC) (2016) Report on internal displacement. Link: http:// bit.ly/37IVaOO
- Owoaje ET, Uchendu OC, Ajayi TO, Cadmus EO (2016) A review of the health problems of the internally displaced persons in Africa. Niger Postgrad Med J 23: 161-171. Link: http://bit.ly/2tytHAK
- UNHCR, NHRC and FEMA (2015) Protection Monitoring Report on IDP sites in the federal Capital Territory. Link: http://bit.ly/2ZYV mqG
- Human Rights Watch (2016) Nigeria: Officials Abusing Displace Women, Girls. Link: http://bit.ly/36yO67w
- Ginindza TG, Stefan CD, Tsoka-Gwegweni JM, Dlamini X, Jolly PE, et al. (2017) Prevalence and risk factors associated with sexually transmitted infections (STIs) among women of reproductive age in Swaziland. Infect Agent Cancer 12: 29. Link: http://bit.ly/2FtU25O
- Basera TJ, Takuva S, Muloongo K, Tshuma N, Nyasulu PS (2016) Prevalence and risk factors for self-reported sexually transmitted infections among adults in diepsloot informal settlement, Johannesburg, South Africa.Journal of AIDS Clinical Research 7: 539. Link: http://bit.ly/ 2FxI36Z
- Raj R, Gupta V, Pathak M, Sreenivas V, Sood S, et al. (2017) What puts them at risk? A cross-sectional case-control survey of demographic profile and sexual behaviour of patients with sexually transmitted infections at a tertiary care center in North India. Indian J Sex Transm Dis AIDS 38: 22–36. Link: http:// bit.ly/36A6DQA
- Saroj RK, Murthy KN, Kumar M, Kumar A (2016) Case Control study of STI patients and its associated risk factors. Global journal of medicine and public health 5: 8. Link: http://bit.ly/35oRL6o
- Menéndez C, Castellsagué X, Renom M, Sacarlal J, Quintó L, et al. (2010) Prevalence and Risk Factors of Sexually Transmitted Infections and Cervical Neoplasia in Women from a Rural Area of Southern Mozambique. Infect Dis Obstet Gynecol 2010 pii: 609315. Link: http://bit.ly/39PSktw
- Hughes G1, Catchpole M, Rogers PA, Brady AR, Kinghorn G, et al. (2000) Comparison of risk factors for four sexually transmitted infections: results from a study of attenders at three genitourinary medicine clinics in England. Sex Transm Infect 76: 262-267. Link: http://bit.ly/36y3lxj
- Park JJ, Seo YB, Jeong S, Lee J (2017) Prevalence of and Risk Factors for Sexually Transmitted Infections among Korean Adolescents under Probation.J Korean Med Sci 32: 1771-1778. Link: http://bit.ly/2Q QuaX3
- Fagbamigbe AF, Adebayo SB, Idemudia E (2016) Marital status and HIV prevalence among women in Nigeria: Ingredients for evidence-based programming. Int J Infect Dis 48: 57–63. Link: http://bit.ly/2N3 MMlg
- Maina AN (2011) Prevalence of and risk factors for sexually transmitted infections among women attending family planning clinic at Kenyatta National Hospital, Nairobi. Link: http://bit.ly/35oUQDu
- National Emergency Management Agency (NEMA) (2016) Displacement Tracking Matrix (DTM) Round VIII Report. Link: http://bit.ly/39IvJii
- WFP and UNICEF (2016) Nigeria Humanitarian Situation Report – a Co Situation Report. Link: http:// bit.ly/35vsbg3
- WHO (2013) Report on global sexually transmitted infection surveillance? Link: http://bit.ly/2SZBySx
- WHO (2013) Sexually transmitted infections: The importance of a renewed commitment to STI prevention and control in achieving global sexual and reproductive health? Geneva. Link: http://bit.ly/ 2N3N4sb
Credits: Ukwajiunor JI, Abanobi OC, Ebirim CIC, Ibe SNO, Nwachukwu CC (2020) Risk Factors of Sexually Transmitted Infections among Women of ChildBearing Age in IDP camps in Abuja. Arch Community Med Public Health 6(1): 012-019. DOI: 10.17352/2455-5479. 000063
[mks_button size=”small” title=”Download the PDF” style=”squared” url=”https://clinicalhealthjournal.com/wp-content/uploads/2020/10/Risk-Factors-of-Sexually-Transmitted-Infections-among.pdf” target=”_self” bg_color=”#000000″ txt_color=”#FFFFFF” icon=”” icon_type=”” nofollow=”0″]






