

Alex M Trafford, Yochai Schonmann, Teng-Chou Chen, Alexander Egeberg, Rosa Parisi, Evangelos Kontopantelis, Ting-Chun Wang, Martin K Rutter, Li-Chia Chen, Tjeerd van Staa, Meng-Sui Lee, Khalaf Kridin, Arnon D Cohen, Kin-Wei A Chan, Alison K Wright, Christopher E M Griffiths, Darren M Ashcroft on behalf of the
Global Psoriasis Atlas
Abstract
Background
Psoriasis is a chronic inflammatory skin disease, and the risk of developing cancer has been postulated due to the presence of several plausible underlying mechanisms. Understanding the association between psoriasis and cancer is imperative to the provision of optimal psoriasis care.
Objectives
To examine the risk of developing cancer in individuals with psoriasis.
Methods
Population-based cohort studies were conducted in Denmark, England, Israel and Taiwan through the use of linked electronic health records. Individuals aged at least 18 years with a diagnosis of psoriasis in the country-specific study period were matched with up to six comparators with no record of psoriasis prior to the index date. Country-specific hazard ratios for the risk of cancer development overall and for 26 site-specific cancers between individuals with and without psoriasis were calculated through Cox regression. Country-specific estimates were pooled using random effects modelling.
Results
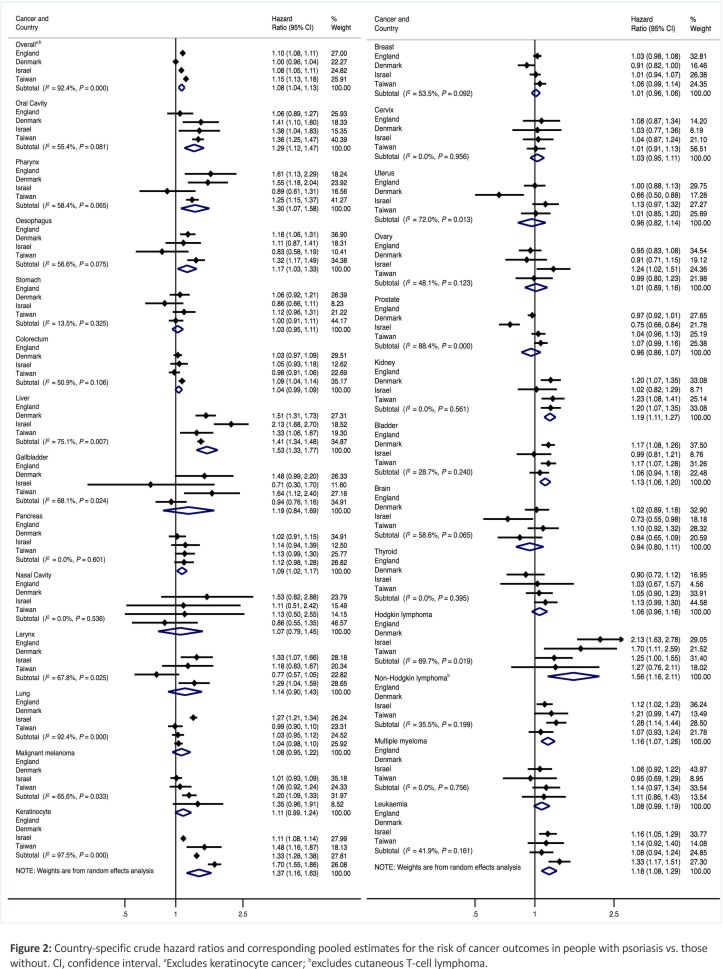
We included 702 022 individuals with psoriasis and 4 185 342 matched comparators. In models implicitly controlled for age, sex and calendar time by matching, there was a small association between psoriasis and cancer overall [pooled HR (pHR) 1.08, 95% confidence interval (CI) 1.04–1.13; I2 = 92.4%]. Adjustment for potential confounding factors resulted in a slight attenuation of risk (pHR 1.05, 95% CI 1.01–1.09; I2 = 81.2%). When restricted to those with moderate-to-severe psoriasis, the risk of cancer overall was slightly higher (pHR 1.16, 95% CI 1.04–1.28; I2 = 92.8%) than in confounder-adjusted models (pHR 1.09, 95% CI 1.03–1.15; I2 = 60.6%). Associations with psoriasis were present for oral cavity (pHR 1.29, 95% CI 1.12–1.47; I2 = 55.4%), pharynx (pHR 1.30, 95% CI 1.07–1.58; I2 = 58.4%), oesophagus (pHR 1.17, 95% CI 1.03–1.33; I2 = 56.6%), liver (pHR 1.53, 95% CI 1.33–1.77; I2 = 75.1%), pancreas (pHR 1.09, 95% CI 1.02–1.17; I2 = 0.0%), kidney (pHR 1.19, 95% CI 1.11–1.27; I2 = 0.0%), bladder (pHR 1.13, 95% CI 1.06–1.20; I2 = 28.7%) and keratinocyte cancers (pHR 1.37, 95% CI 1.16–1.63; I2 = 97.5%), and Hodgkin lymphoma (pHR 1.56, 95% CI 1.16–2.11; I2 = 69.7%), non-Hodgkin lymphoma (pHR 1.16, 95% CI 1.07–1.26; I2 = 35.5%) and leukaemia (pHR 1.18, 95% CI 1.08–1.29; I2 = 41.9%). Site-specific associations generally persisted, with slight risk exacerbations and additional associations for lung and ovarian cancers, when limited to people with moderate-to-severe psoriasis.
Conclusions
Psoriasis was associated with an increased risk of developing 14 of 26 investigated site-specific cancers, including cancers with a poor prognosis, such as liver, lung and oesophageal cancer. Our findings can be used to reinforce cancer prevention strategies in psoriasis care.
Lay Summary
Psoriasis is a long-term skin condition that affects about 60 million people worldwide. People with psoriasis are at risk of other health problems like joint pain and heart disease. Yet, their risk of developing cancer is not well understood. Other studies have investigated this, but the results have been inconsistent.
In this study, we aimed to understand the association between psoriasis and cancer. We examined databases containing health information in Denmark, England, Israel and Taiwan. We compared over 700,000 people with psoriasis and over 4 million people without it. We found that people with psoriasis had a slightly higher risk of developing cancer than people without it. This risk was slightly higher in people with more severe psoriasis. Cancers of the mouth, pharynx (throat), oesophagus, liver, pancreas, kidney and bladder were more likely in people with psoriasis. They were also more likely to develop a particular type of skin cancer. Some blood cancers were also more likely in people with psoriasis. The risk of these cancers was higher in people with more severe psoriasis.
Our findings suggest that there is an increased risk of cancer in people with psoriasis. This information should be used to ensure people with psoriasis get the best care.
What is already known about this topic?
- Several mechanisms make an association between psoriasis and cancer plausible, including chronic inflammation and the use of immunomodulatory therapies.
- Previous estimates of cancer risk in people with psoriasis vary, particularly for site-specific cancers, resulting in a poor understanding of the association for many cancers.
- Previous studies have been inconsistent in their design, with variation in the population with psoriasis considered, methodologies used to produce estimates and the range of cancers considered.
What does this study add?
- Psoriasis was associated with an increased risk of developing cancer overall and with 14 site-specific cancers derived from population-based cohort studies from 4 different countries.
- Associations generally persisted, with risk exacerbated, when limited to people with moderate-to-severe psoriasis.
- Psoriasis is associated with specific cancers, and this should be recognized in order to guide optimal psoriasis care pathways.
Psoriasis is an immune-mediated inflammatory skin disease that affects at least 60 million people worldwide.1 The prevalence of psoriasis varies geographically, occurring more frequently in high-income countries and in regions with older populations and least frequently in East Asian countries (2.3% in Israel, 2.3% in Denmark, 1.9% in the UK, 0.1% in Taiwan).1 In addition to the cutaneous manifestations of the condition, psoriasis is also associated with a complex web of comorbidities.2
Cancer is acknowledged as an important comorbidity in several chronic conditions, including Crohn disease and diabetes mellitus.3,4 In psoriasis, several different mechanisms may play a role, including systemic inflammation increasing cancer risk through DNA damage and the production of a pro-tumorigenic macroenvironment; immunomodulatory and phototherapies commonly used in the treatment of moderate-to-severe psoriasis; and increased incidence and prevalence of established cancer risk factors, including smoking, alcohol consumption and obesity.5–7
Despite this, cancer risk in individuals with psoriasis continues to lack clarity, with two meta-analyses reporting notable heterogeneity in estimates, particularly for site-specific cancers.8,9 This is likely to stem from inconsistencies in study design, including psoriasis population sources, risk assessment methods and confounder adjustments. Using a common study design across four countries (England, Denmark, Israel, Taiwan), our study aimed to minimize heterogeneity by examining incident cancer risk in individuals with psoriasis and to determine whether cancer risk varies with disease severity.
Patients and methods
Data sources
The data sources used included the Danish National Patient Registry (DNPR; Denmark); the Clinical Practice Research Datalink (CPRD) GOLD and Aurum (UK);10,11 the Clalit health Services database (Israel); and the Taiwan National Health Insurance (NHI) database (Taiwan). All databases collected information on demographics, diagnoses and prescriptions/procedures either as part of the maintenance of electronic health records (Denmark and UK) or for insurance administration purposes (Israel and Taiwan). Further details regarding the data sources used, including information on ethical approval, are provided in Appendix S1 (see Supporting Information).
Study population
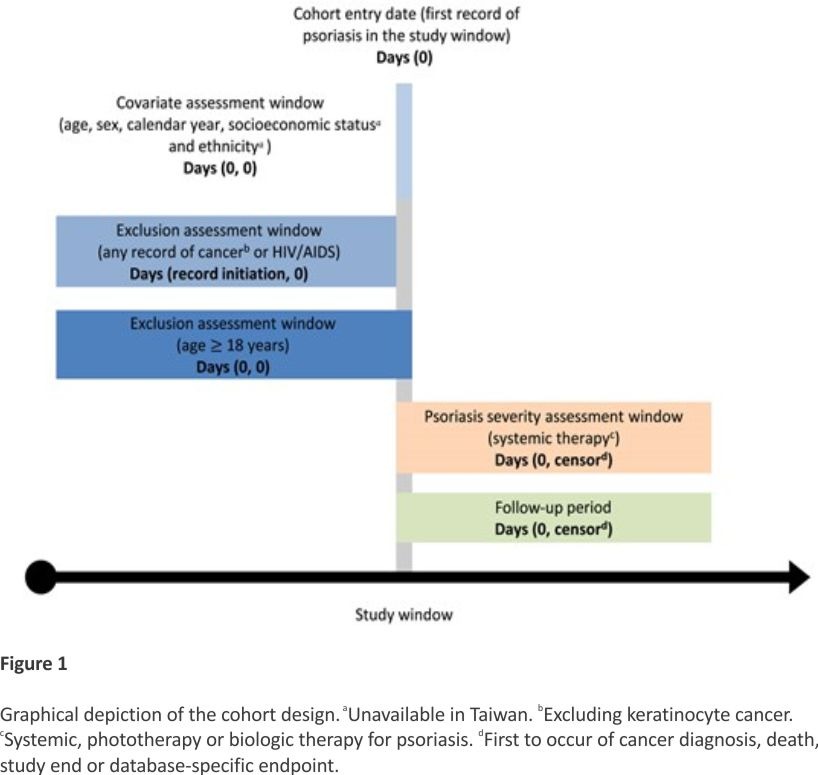
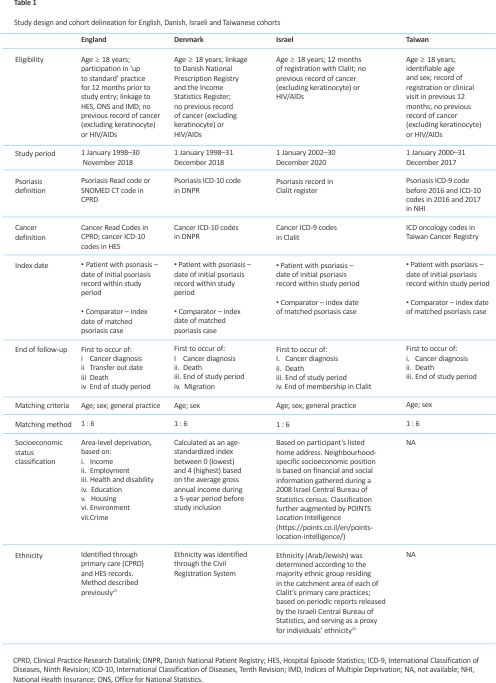
This study applied a common protocol approach; hence, we describe the shared details and outline the between-country differences in Table 1. In summary, individuals with a record of psoriasis in the study period were matched to comparator patients with no record of psoriasis prior to index, based on a minimum of exact age and sex. The date of the first psoriasis record in the study period was defined as the index date for patients with psoriasis, with comparators designated the index date of their matched patient. Patients were followed from index date to the first occurrence of cancer diagnosis, death, end of study period or database-specific endpoint (Figure 1). As cancer diagnosis was used as an endpoint, where a patient experienced more than one diagnosis, only the first cancer to occur was considered. Patients with any cancer (excluding keratinocyte) or HIV/AIDS record prior to study entry were excluded. Cohort delineation for each country is outlined in Figure 1.
Outcomes included any cancer diagnosis and site-specific cancer diagnosis during the follow-up period. Any cancer diagnosis excluded keratinocyte cancers due to potential detection bias in the group with psoriasis. Cutaneous T-cell lymphoma (CTCL) records were excluded from any cancer and non-Hodgkin lymphoma counts due to reported misclassification of CTCL in psoriasis.12 For the same reason, CTCL was not considered as an outcome of interest. Breast, cervical, uterine and ovarian cancer outcomes were only considered in women. Prostate cancer was only considered in men. Details on the data sources and methods used to identify cancer diagnosis in the different countries are provided in Table 1.
Psoriasis severity
Using a validated approach,13,14 patients were defined as having moderate-to-severe psoriasis if receiving systemic therapy (acitretin, apremilast, ciclosporin, etretinate, fumaric acid, hydroxycarbamide or methotrexate), phototherapy or biologic therapy (adalimumab, brodalumab, certolizumab, efalizumab, etanercept, guselkumab, infliximab, ixekizumab, secukinumab or ustekinumab). Moderate-to-severe status was defined at the first date of receiving a relevant therapy, with individuals considered to have moderate-to-severe disease from that point onwards. Comparators were designated an index date matching the date of therapy receipt for their respective case.
Covariates
Variables considered as potential confounders included age, sex, calendar time, ethnicity and socio- economic status. Age, sex and calendar time were accounted for in the matching. Details on ascertainment of ethnicity and socioeconomic status in England, Denmark and Israel are outlined in Table 1.
Statistical analysis
Characteristics of individuals with psoriasis and comparators at baseline were summarized descriptively. Rates for any cancer and site-specific cancers were calculated per 100 000 person-years (PY). The attributable risk – the difference between absolute risks in the patients with psoriasis and their comparators – was calculated, with a positive risk difference indicating excess risk due to psoriasis. Cox proportional hazard models, stratified to account for matching, were used to calculate hazard ratios (HRs) and corresponding 95% confidence intervals (CIs) separately for the respective countries, with Schoenfeld residuals used to assess the proportional hazards assumption. Country-specific estimates were meta-analysed to produce pooled estimates using the Der Simonian–Laird random-effects method. Heterogeneity was measured through the I2 statistic. Adjustment for multiple comparisons was not applied as comparisons were complementary, and to prioritize minimization of type II error, particularly with the rarer cancer outcomes.
Crude models were implicitly adjusted by age, sex and calendar time through matching. Confounder-adjusted models also included measures of socioeconomic status and ethnicity (categorized according to the study country in question). Owing to limitations in data availability, confounder-adjusted models are not presented for Taiwan.
Several sensitivity analyses were performed to assess the robustness of the main findings. Details of the methods followed in each sensitivity analysis and respective rationales are included in Table S1 (see Supporting Information).
Results
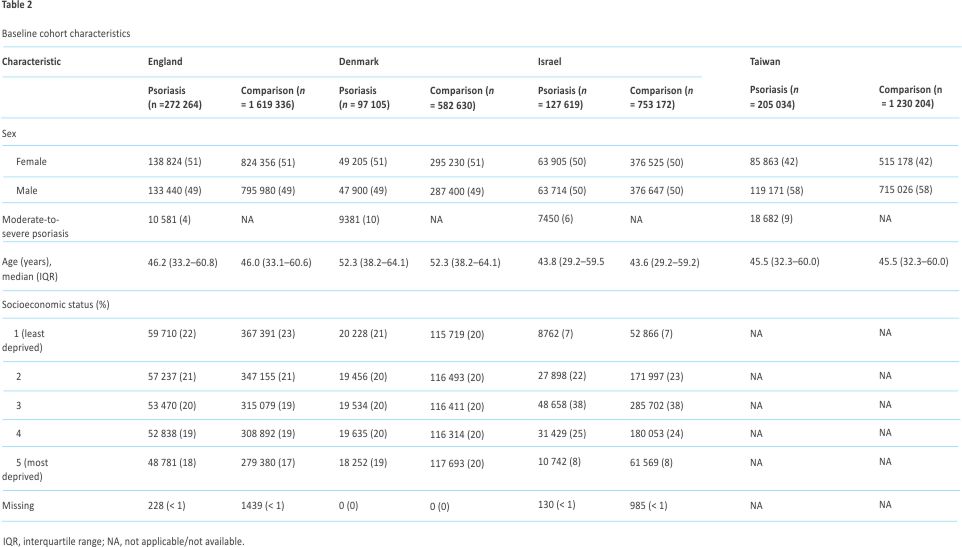
Patient characteristics are outlined in Table 2. The study included 272 264 individuals with psoriasis and 1 619 336 matched comparison patients in England; 205 034 individuals with psoriasis and 1 230 204 comparators in Taiwan; 127 619 individuals with psoriasis and 753 172 comparators in Israel; and 97 105 patients with psoriasis and 582 630 comparators in Denmark. Sex distribution was balanced in England, Denmark and Israel, while in Taiwan there were slightly more men (58%) than women (42%). Median age ranged from 43 (Israel) to 52 (Denmark) years. Details of the ethnicity of individuals is provided in Table S2 (see Supporting Information). In England, 81% of patients with psoriasis were White, 3% were Asian, 1% were Black and 1% were registered as ‘other’; the ethnicity of 14% of patients was unknown. In Denmark, 95% of patients with psoriasis were Danish, 3% were other European, 1% were Asian, < 1% were African and < 1% were recorded as ‘other/unknown’ (see Table S2 for more detail). In Israel, 83% of patients with psoriasis were Jewish and 17% were Arab. The proportion of patients with psoriasis classified as having moderate-to-severe disease at baseline was higher in Denmark (10%) and Taiwan (9%), and marginally lower in Israel (6%) and England (4%).
The incidence rate of all cancer was higher in people with psoriasis than comparators without psoriasis in England (903.2 vs. 839.0 cases per 100 000 PY), Israel (716.9 vs. 655.7 per 100 000 PY) and Taiwan (811.8 vs. 707.5 per 100 000 PY; see Table S3). In Denmark, the incidence of cancer was slightly lower in people with psoriasis than people without psoriasis (1126.1 vs. 1140.6 per 100 000 PY). This pattern was consistent for individual cancer sites (stomach, lung, breast, bladder and multiple myeloma). Across all four countries, patients with psoriasis had higher incidence rates of cancers of the oral cavity, liver, pancreas, keratinocytes, cervix and kidney, and Hodgkin lymphoma, non-Hodgkin lymphoma and leukaemia.
Comparing absolute risks by psoriasis severity, patients with moderate-to-severe psoriasis had consistently higher rates of all cancers and for individual cancer sites than people with mild psoriasis and people without psoriasis (see Table S4). The difference in rates between patients with moderate-to-severe and mild psoriasis was most pronounced for colorectum, lung, keratinocyte, breast and prostate cancer.
Overall cancer
There was a modest positive association between having psoriasis and overall cancer in crude models [pooled HR (pHR) 1.08, 95% CI 1.04–1.13; I2 = 92.4%], with increased risks observed in England, Israel and Taiwan (see Figure 2). While the association persisted across confounder-adjusted models (see Figure S1), the pooled estimate was attenuated (pHR 1.05, 95% CI 1.01–1.09; I2 = 81.2%). There was no association between having psoriasis and overall cancer in Denmark.
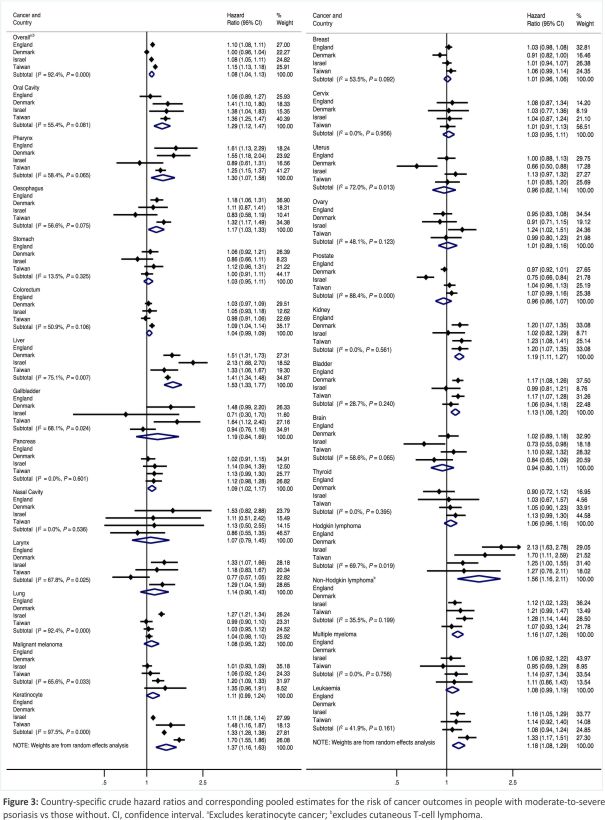
In individuals with moderate-to-severe psoriasis, the risk of overall cancer was slightly higher in crude (pHR 1.16, 95% CI 1.04–1.28) and confounder-adjusted (pHR 1.09, 95% CI 1.03–1.15) models when compared with all patients with psoriasis (Figure 3, Figure S2).
Solid cancers
In crude models, statistically significant positive associations were found between having psoriasis and the following site-specific cancers: oral cavity (pHR 1.29, 95% CI 1.12–1.47), pharynx (pHR 1.30, 95% CI 1.07–1.58), oesophagus (pHR 1.17, 95% CI 1.03–1.33), liver (pHR 1.53, 95% CI 1.33–1.77), pancreas (pHR 1.09, 95% CI 1.02–1.17), kidney (pHR 1.19, 95% CI 1.11–1.27) and bladder (pHR 1.13, 95% CI 1.06–1.20). Estimates were generally consistent in confounder-adjusted models; however, significant associations were no longer present for oral cavity, pharyngeal, oesophageal and pancreatic cancers.
When restricted to moderate-to-severe psoriasis, increased risks were found for the following cancers in crude models: oral cavity (pHR 1.62, 95% CI 1.41–1.86), pharynx (pHR 1.50, 95% CI 1.29–1.74), oesophagus (pHR 1.33, 95% CI 1.12–1.58), liver (pHR 1.70, 95% CI 1.26–2.28), pancreas (pHR 1.22, 95% CI 1.05–1.43), larynx (pHR 1.51, 95% CI 1.15–1.97), lung (pHR 1.28, 95% CI 1.10–1.48) and ovary (pHR 1.26, 95% CI 1.03–1.55).
For all cancer associations, the risk was exacerbated when restricted to those with moderate-to-severe psoriasis. In confounder-adjusted models, significant associations remained for oral cavity, pharynx, liver, pancreas, lung and ovarian cancer. A small but reduced risk of prostate cancer was found (pHR 0.82, 95% CI 0.73–0.93). The incidence of gallbladder and nasal cavity cancer in patients with moderate-to-severe psoriasis was not assessed due to insufficient outcome numbers.
Skin cancers
In all individuals with psoriasis, a moderately increased risk of keratinocyte cancer was found in crude (pHR 1.37, 95% CI 1.16–1.63) and confounder-adjusted (pHR 1.25, 95% CI 1.05–1.49) models. No association was found with malignant melanoma.
The risk of keratinocyte cancer was higher in patients with moderate -to-severe psoriasis, with positive associations in crude (pHR 1.42, 95% CI 1.18–1.70) and confounder-adjusted (pHR 1.25, 95% CI 1.18–1.33) models. As in all psoriasis, there was no association with malignant melanoma.
Lymphatic and haematopoietic tissue cancers
An increased risk of Hodgkin lymphoma was found in crude (pHR 1.56, 95% CI 1.16–2.11) and confounder-adjusted (pHR 1.60, 95% CI 1.17–2.20) models for those with vs. those without psoriasis. Increased risks in crude and confounder-adjusted models were similarly found for non-Hodgkin lymphoma (excluding CTCL) and leukaemia. No association was found with multiple myeloma.
Increased risks of Hodgkin lymphoma (pHR 1.99, 95% CI 1.42–2.79), non-Hodgkin lymphoma (pHR 1.43, 95% CI 1.15–1.77) and leukaemia (pHR 1.61, 95% CI 1.03–2.49) were also found in crude models for moderate-to-severe psoriasis. Associations persisted in confounder-adjusted models.
Attributable risk
Excess cancer risks in people with psoriasis are presented in Table S4. Overall, 10% of cancers were attributable to psoriasis (10% in England, 10% in Israel, 13% in Taiwan). The excess risk associated with psoriasis differed by cancer type, with the largest impact observed for Hodgkin lymphoma (35%), followed by liver (29%), oral cavity (23%), pharynx (21%), keratinocyte (19%), kidney (18%), oesophagus (16%), leukaemia (16%), non-Hodgkin lymphoma (15%), larynx (13%), bladder (12%) and lung cancer (11%).
Sensitivity analyses
The patterns seen in the primary analysis were consistent across all sensitivity analyses (exclusion of individuals with a history of psoriatic arthritis; restriction to incident psoriasis cases only; and exclusion of patients with < 12 months of follow-up) (see Table S5). A modest positive association between psoriasis and overall cancer risk was observed in England, Israel and Taiwan, but not Denmark, both in crude and confounder-adjusted models, with slightly higher risk in individuals with moderate-to-severe psoriasis. The increased risk of several site-specific cancers – including those of the oral cavity, pharynx, liver, kidney and keratinocytes, and Hodgkin and non-Hodgkin lymphomas – was similarly observed.
Discussion
In this international study involving population-based cohorts from four countries, we found an increased risk of several site-specific cancers in individuals with psoriasis, including oral cavity, pharyngeal, oesophageal, liver, pancreatic, kidney, bladder, keratinocyte cancers, Hodgkin lymphoma, non-Hodgkin lymphoma and leukaemia. Site-specific associations largely persisted when restricted to those with moderate-to-severe psoriasis, with additional associations noted for lung, laryngeal and ovarian cancers. Conversely, a reduced risk was only found for prostate cancer.
This study builds on two systematic reviews and meta-analyses of cancer risk in psoriasis.8,9 Of the seven solid cancers found to be associated with psoriasis in this study, five align with prior findings, although risk estimates were consistently more modest. Further-more, while prior studies have reported associations in conflicting directions, such a phenomenon did not occur in this study. Most associations with solid organ cancers persisted in moderate-to-severe psoriasis, except for bladder and renal cancers. While few prior studies have focused on this subgroup, the slightly elevated risks in moderate-to-severe psoriasis vs. those of all psoriasis in this study are consistent with previous findings.8
Previous studies and meta-analyses on malignant melanoma risk in psoriasis have been conflicting. 8,9,15,16 While the pooled estimate in this study also showed no overall association, country-specific estimates varied: there was little-to-no change in risk in England and Denmark but approximately a 30% increased risk in Israel and Taiwan.
The mechanistic underpinning and causal pathway of the association between psoriasis and cancer are not fully established (Figure S3; see Supporting Information); however, several risk factors may have a role, including genetic factors, lifestyle factors, comorbidities and treatments for psoriasis. An overview of these risk factor relationships is provided in Appendix S2 (see Supporting Information).
While an increased risk of cancer in people with psoriasis was observed in England, Israel and Taiwan, there was no association in Denmark. This may be attributed to the smaller sample size of the Danish cohort and higher cancer incidence in the general population. Denmark’s estimated cancer incidence rate is higher than the European Union average and the highest among the Nordic countries.17 According to 2022 data from the World Cancer Research Fund, Denmark had the highest global cancer incidence rate out of the 185 countries (including the UK and Israel) when excluding nonmelanoma skin cancer and the third highest incidence rate when all cancers were included.18
The higher incidence of cancer in Denmark may be attributed to several factors, including free national screening programmes implemented in hospital and general practitioners, earlier detection, comprehensive registry-based recording of screening and diagnoses, genetic background, and the ‘cancer–cold’ hypothesis.17,19
The consistent association between psoriasis and several site-specific cancers highlights the need for cancer screening to receive greater recognition in psoriasis care. The clinical relevance of such associations is further demonstrated by findings of excess case numbers when considering absolute risk for cancers with poor prognosis, such as lung and liver cancer. Previous work has demonstrated the role of the urgent suspected cancer referral pathway in reducing cancer morbidity.20 The recognition of people with psoriasis as an at-risk cancer group may increase the use of this pathway, with potential improvement in outcomes through earlier diagnosis.
Given the potential for psoriasis to exacerbate cancer risk through increased tumour promotion and progression (see Appendix S2), it is of utmost importance that those with the condition receive support in addressing lifestyle factors with genotoxic effects. Smoking and alcohol consumption are clear targets in this regard, and the importance of addressing such factors is evidenced by findings of excess lung cancer cases in England and liver cancer cases in Denmark and Taiwan. The international nature of this study also highlights the importance of population-specific risk factors. Of particular note in this respect is betel quid, a common carcinogenic chewing product in Asian populations, 21 which may explain the increased risk of oral cavity and oesophageal cancers in Taiwan. Future research should aim to quantify the role of these lifestyle factors in reported cancer associations.
One key strength of this study is the use of a common protocol and shared coding syntax across four large population-based cohorts, providing results with a strong degree of generalizability. The large population size not only provides greater precision, but also the power to detect small differences in risk for rarer cancers.
Despite the implementation of a common study protocol, variation in the proportion of patients classified with moderate-to-severe psoriasis may, in part, be related to differences in availability of proxy measures for defining psoriasis severity in the different databases. Patients with more severe or extensive psoriasis are typically referred from primary care to secondary care and private clinics. The twofold difference in moderate-to-severe psoriasis seen in England vs. the other countries (4% vs. 6%, 9% and 10%) could be affected by not having access to hospital prescribing data and as such relies on these prescriptions being recorded in the general practice patient record. Substantial hetero- geneity between country-specific estimates was noted for several site-specific outcomes. The cause of such heterogeneity is likely to be twofold: (i) intercountry differences in database structure and recording practices; and (ii) the potential for slight differences in recording practices. Importantly, heterogeneity in site-specific risk estimates may also reflect population-specific cancer patterns.
A limitation of using routinely collected data is the lack of data on direct psoriasis severity measures such as body surface area, Psoriasis Area Severity Index, Dermatology Life Quality Index, Physician’s Global Assessment or location of involve- ment.22 However, we used a validated approach where prescriptions for systemic therapy and biologics are considered surrogate markers for moderate-to-severe psoriasis in electronic health record and administrative databases.13,14 While using prescription information for defining severity could result in some misclassification, this would not affect our results for cancer risk in all psoriasis patients. In addition, while the omission of lifestyle factors may be considered a limitation, such an omission is not without reason. As the mechanistic underpinning of the association between psoriasis and cancer is unclear, it is crucial to first establish what the risk of developing different types of cancers among people with psoriasis is to provide a foundation for understanding the potential link between the two conditions.
We found an association between psoriasis and several incident site-specific cancers. These findings emphasize the need to reinforce cancer prevention strategies in the care of patients with psoriasis so as to reduce the cancer burden.
Acknowledgements
The authors acknowledge the key role played by the Global Psoriasis Atlas (GPA) Collaborating Organisations in the establishment and organization of the GPA: the International Psoriasis Council; the International Federation of Psoriasis Associations; and the International League of Dermatological Societies. We are grateful for the enthusiastic collaboration of all GPA Board of Governors, Steering Committee members, and regional and national coordinators. The views and opinions expressed herein are those of the authors and do not necessarily reflect those of the GPA collaborating organizations or funders. More details on the GPA are available at https://www. globalpsoriasisatlas.org/.
Funding sources
This study was funded by the International League of Dermatological Societies (ILDS) on behalf of the Global Psoriasis Atlas. Funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Conflicts of interest
All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/disclosure-of-interest/and declare the following. A.E. reports receiving grants from AbbVie, the Danish National Psoriasis Foundation, Eli Lilly, Janssen, Kgl Hofbundtmager Aage Bangs Foundation, Novartis, Pfizer and the Simon Spies Foundation. A.E. has also received consulting fees from AbbVie, Almirall, Bristol Myers Squibb, Dermavant, Eli Lilly, Galderma, Janssen, LEO Pharma, Mylan, Novartis, Pfizer, Samsung Bioepis, UCB and Union Therapeutics. A.E. has received payment for presentations with AbbVie, Almirall, Bristol Myers Squibb, Dermavant, Eli Lilly, Galderma, Janssen, LEO Pharma, Mylan, Novartis, Pfizer, Samsung Bioepis and UCB. M.K.R. reports receiving consulting fees from Cell catapult and modest owning of shares in GSK. M.K.R. also reports acting as Chair for Diabetes UK, professional conference organizing committee (2021–22) and Diabetes UK, Diabetes Research Steering Group 6 (2021–). T.v.S. reports payment for expert testimony from the UK Government Legal department related to pregnancy tests. A.D.C. has received research grants from Janssen, Novartis and AbbVie. A.D.C. has also served as a consultant, advisor or speaker for AbbVie, Amgen, Boehringer Ingelheim, Dexcel Pharma, Janssen, Eli Lilly, Neopharm, Novartis, Perrigo, Pfizer and Rafa. K.-W.A.C. reports receiving grants from Bayer, Takeda, Amgen, Boehringer Ingelheim, MundiPharma, Merck Sharp and Dohme and GlaxoSmithKline. K.-W.A.C. has additionally received consulting fees from Bayer and payment from Amgen. C.E.M.G. reports receiving grants from the LEO Foundation and Almirall. C.E.M.G. has also received consulting fees from Artax, Boehringer Ingelheim, BMS, Johnson & Johnson, Novartis, Nxera, Sun Pharma, Takeda and UCB. C.E.M.G. has been paid for presentations by Almirall, Boehringer Ingelheim, BMS, Eli Lilly, Glenmark, Johnson & Johnson, Novartis and UCB. D.M.A. reports receiving grants from the LEO Foundation, AbbVie, Almirall, Celgene, Eli Lilly, Novartis, UCB and Janssen. The other authors declare no conflicts of interest.
Data availability
Electronic health records are, by definition, considered sensitive data and cannot be shared via the public. Access to the data used in this study may be made available through successful application to country-specific sources. The reporting of this study conforms to the STROBE statement. The checklist can be found in Table S6 (see Supporting Information).
Ethics statement
England: the study was approved by the Independent Scientific Advisory Committee (ISAC) for Medicines and Healthcare Products Regulatory Agency database research (ISAC approval 19_089R). Denmark: the project was approved by the Danish Data Protection Agency and registered with the Capital Region’s inventory (VD-2018-286). Israel: the project received institutional ethical approval (no. 0212-17-COM). Taiwan: the study was approved by the Institutional Review Board of the National Taiwan University Hospital (approval no: 201808083W).
Patient consent
Not applicable.
Supporting Information
Additional Supporting Information may be found in the online version of this article at the publisher’s website.
References
1. Parisi R, Iskandar IYK, Kontopantelis E et al. National, regional, and worldwide epidemiology of psoriasis: systematic analysis and modelling study. BMJ 2020; 369:m1590.
2. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet 2021; 397: 1301–15.
3. Canavan C, Abrams KR, Mayberry J. Meta-analysis: colorectal and small bowel cancer risk in patients with Crohn’s disease. Aliment Pharmacol Ther 2006; 23:1 097– 104.
4. Shikata K, Ninomiya T, Kiyohara Y. Diabetes mellitus and cancer risk: review of the epidemiological evidence. Cancer Sci 2013; 104 :9–14.
5. Armstrong AW, Harskamp CT, Dhillon JS, Armstrong EJ. Psoriasis and smoking: a systematic review and meta-analysis. Br J Dermatol 2014; 170:304–14.
6. Parisi R, Webb RT, Carr MJ et al. Alcohol-related mortality in patients with psoriasis. JAMA Dermatol 2017; 153:1256–62.
7. Armstrong AW, Harskamp CT, Armstrong EJ. The association between psoriasis and obesity: a systematic review and meta-analysis of observational studies. Nutr Diabetes 2012; 2:e54.
8. Trafford AM, Parisi R, Kontopantelis E et al. Association of psoriasis with the risk of developing or dying of cancer. JAMA Dermatol 2019; 155:1390–403.
9. Vaengebjerg S, Skov L, Egeberg A, Loft ND. Prevalence, incidence, and risk of cancer in patients with psoriasis and psoriatic arthritis. JAMA Dermatol 2020; 156:421–9.
10. Herrett E, Gallagher AM, Bhaskaran K et al. Data resource profile: Clinical Practice Research Datalink (CPRD). Int J Epidemiol 2015; 44:827–36.
11. Wolf A, Dedman D, Campbell J et al. Data resource profile: Clinical Practice Research Datalink (CPRD) Aurum. Int J Epidemiol 2019; 48:1740.
12. Trafford AM, Parisi R, Rutter MK et al. Concordance and timing in recording cancer events in primary care, hospital and mortality records for patients with and without psoriasis: a population-based cohort study. PLOS ONE 2021; 16:e0254661.
13. Egeberg A, Mallbris L, Gislason GH et al. Risk of multiple sclerosis in patients with psoriasis: a Danish nationwide cohort study. J Invest Dermatol 2016; 136: 93–8.
14. Egeberg A, Gyldenløve M, Zachariae C, Skov L. Validation of psoriasis severity classification based on use of topical or systemic treatment. J Eur Acad Dermatol Venereol 2018; 32:e4–5.
15. Boffetta P, Gridley G, Lindelöf B. Cancer risk in a population-based cohort of patients hospitalized for psoriasis in Sweden. J Invest Dermatol 2001; 117:1531–7.
16. Li W-Q, Han J, Cho E et al. Personal history of psoriasis and risk of incident cancer among women: a population-based cohort study. Br J Dermatol 2016; 174:1108–11.
17. European Cancer Inequalities Registry and OECD. Country Cancer Profile 2023 – Denmark. Available at: https://www.oecd.org/content/dam/oecd/en/publications/reports/2023/02/eu-country-cancer-profile-denmark-2023_89208faa/ ee590fe8-en.pdf
18. World Cancer Research Fund. Global Cancer Data by Country. Available at: https://www. wcrf.org/preventing-cancer/ cancer-statistics/global-cancer-data-by-country/#global-cancer-incidence-both-sexes
19. Voskarides K. The “cancer–cold” hypothesis and possible extensions for the Nordic populations. Scand J Public Health 2019; 47: 477 – 81.
20. Round T, Gildea C, Ashworth M, Møller H. Association between use of urgent suspected cancer referral and mortality and stage at diagnosis: a 5-year national cohort study. Br J Gen Pract 2020; 70:e389–98.
21. Sharan RN, Mehrotra R, Choudhury Y, Asotra K. Association of betel nut with carcinogenesis: revisit with a clinical perspective. PLOS ONE 2012; 7:e42759.
22. Strober B, Ryan C, van de Kerkhof P et al. Recategorization of psoriasis severity: Delphi consensus from the International Psoriasis Council. J Am Acad Dermatol 2020; 82:117–22.
23. Wright AK, Kontopantelis E, Emsley R et al. Life expectancy and cause-specific mortality in type 2 diabetes: a population-based cohort study quantifying relation-ships in ethnic subgroups. Diabetes Care 2017; 40:338–45.
24. Falah G. Living together apart: residential segregation in mixed Arab–Jewish cities in Israel. Urban Stud 1996; 33:823–57.
Credits: Alex M Trafford, Yochai Schonmann, Teng-Chou Chen, Alexander Egeberg, Rosa Parisi, Evangelos Kontopantelis, Ting-Chun Wang, Martin K Rutter, Li-Chia Chen, Tjeerd van Staa, Meng-Sui Lee, Khalaf Kridin, Arnon D Cohen, Kin-Wei A Chan, Alison K Wright, Christopher E M Griffiths, Darren M Ashcroft, on behalf of the Global Psoriasis Atlas, Psoriasis and risk of 26 cancers: pooled population-based cohort studies from Denmark, England, Israel and Taiwan, British Journal of Dermatology, Volume 194, Issue 1, January 2026, Pages 67–76, https://doi.org/10.1093/bjd/ljaf399