

Okereke, Promise Udohchukwu BDSa,b,c,*; Obiora, Benjamin Chidum MBBSd; Obu, Franklin Chibueze MBBSd; Ochi, Chizoba Judith MBBSd; Odigidawu, Onyebuchi Victor MBBSd; Okereke, Obumneme Wisdom BDSb,e; Umeh, Chukwuemeka Victor MBBSf; Tola, Olalekan Simeon MBBSg; Ibekwe, SolomonNnayelugo BDSa,h; Nnaji, Uche MBBSi; Ifedibar, Chisom Wisdom MBBSj; Uche, Collins BDSa,k; Nnegboh, Philip Chukwunonso MBBSd; Ogbu, Andrew Chukwuemeka MBBSl; Ogamba, Nzubechukwu MBBSd; Ogunlana, Olaoluwaposi Emmanuel MBBSm
Abstract
Background:
Depression is a prevalent and serious mental health issue, particularly among young adults and medical students. Medical students, due to high academic and emotional stress, are particularly vulnerable to developing depression, which is often unnoticed in its early stages. This study aimed to assess the prevalence and patterns of depression among clinical medical students in a University in Nigeria.
Methods:
A descriptive cross-sectional study was conducted among 230 clinical medical students in their fourth to sixth years of study. The Beck Depression Inventory (BDI) was used to assess depressive symptoms.
Results:
The overall prevalence of depression was 30.8%, with 14.8% reporting moderate depression, 1.3% severe depression, and 0.4% extreme depression. The most frequently cited triggers for depression were academic workload (92.5%) and poor social amenities (60.4%).
Conclusion:
Depression is highly prevalent among medical students, particularly in clinical years, underscoring the need for early screening and mental health interventions.
Introduction
Depression is the fourth leading cause of disability worldwide. It affects an estimated 1 in 15 adults in any given year and 1 in 16 people will experience depression at some point in their life. An estimated 3.8% of the world’s population is said to be affected1,2. Depression can occur at any time but on average, it first appears during the late teens to mid-20s, with women more likely to be affected than men2. It is worthy of note that the risk of depression is more in the most productive years of a person’s life2.
Depression is a significant public health problem in Nigeria and at a prevalence of 3.9%, seven million Nigerians currently suffer from depression3. Several studies conducted in Nigeria have reported a prevalence of depression among young adults, elderly, internally displaced persons as 25%, 26.2%, and 17%, respectively4. The high prevalence of depression reported among this population suggests that depression is a very common occurrence among people who face social adversity and difficulties.
The debilitating effects of this mental illness may not be immediately appreciated by the public because it affects the brain unlike some other illnesses which affect known organ systems and manifest with common symptoms pertaining to those organs. Depression tends to go unnoticed as some of its early symptoms are equally experienced by apparently healthy individuals. As many as two-thirds of people with depression do not realize they have a treatable illness and therefore do not seek professional help5. In addition, persistent ignorance and misperceptions of the disease as a weakness that can be willed or wished away, lead to stigmatization and avoidance of diagnosis among those affected5.
Depression is an age-long disease that was described in man centuries ago, albeit, poorly understood. During the time of Hippocrates, it was called “melancholia” and at that time, the cause was attributed to an imbalance of the four humoral fluids3. It was not until the 19th century that the term “Depression” was used. In the 20th century, classification systems were developed: International Statistical Classification of Diseases and Diagnostic and Statistical Manual of Mental Disorders3.
The etiology of depression has not been completely understood and many theories have been propounded in an attempt to describe it. One of these numerous theories is the effect of stressors4,6. While the aphorism “Life is not a bed of roses” is true for every country and all subsets of the human population, it appears to be “more true” in our country Nigeria. Nigeria still falls under the category of developing nations and as such has a very high poverty rate. Poverty here can be equated to suffering which also has a relationship with stressors4,5.
For many, admission into the university is a time of significant transition and many times transformation. For some, this is also a period of increased stress. Medical students suffer high levels of stress5 which may be caused by one or more of many factors including the fact that they are provided with tremendous amounts of information which they are to memorize6, excessive workload, resultant sleep deprivation7, and professional exams. In addition to this, many medical schools present a rigid environment which tends to foster the spirit of competition in students rather than cooperation, the result being an aggravation of (the already present) stress and tension8. Lloyd and Gartrell9 proved that medical students are more distressed when juxtaposed with the general population.
Researchers have suggested that although the rate of depression among students entering medical school is similar to that among other people of similar ages, the prevalence increases disproportionately over the course of medical school10. In other words, at the beginning of the course, the psychological morbidity of medical students is similar to that of nonmedical students and the general public; however, as they progress through the course their mental health worsens11. A meta-analysis of studies from 43 countries showed that the prevalence of depression among medical students averaged 27.2%12. In another systematic review of 15 research works, the prevalence of depression was higher among medical students and pharmacy students when compared to the general population13. A more recent study of depression among 273 medical students in Addis Ababa showed a prevalence of 51.3%14. Studies have found that under-reporting and under-treatment of depression is common among medical students, with reporting rates as low as 15.7%12 and treatment rates as low as <25%15. This translates to higher rates of suicide ideation amongst medical students, for which one large multi-institution study has reported a prevalence of 11.2%16.
Depression amongst medical students deserves special attention; it not only affects students’ lives in terms of academic performance, dropout, and professional development, but may also have repercussions on patient care in the long run17.
The different challenge that the medical students encounter during their training period may increase their predisposition toward depression, and its consequent problems. Hence, early identification is necessary for forestalling negative outcomes.
Whereas other factors affecting medical students have been identified and studied in previous research, there is a lack of knowledge about clinical depression regarding medical students in the University of Nigeria. The broad topic of clinical depression has received attention, including from the government, but the assumed pattern of presentations among medical students has not been the focus of attention.
Therefore, this study aimed to determine the prevalence, patterns, and the factors associated with depression among clinical medical students in a major medical college in southeastern Nigeria.
Materials and methods
This descriptive cross-sectional study was conducted among clinical medical students at a university in Nigeria, one of the major medical schools in Southeast Nigeria. The study population included 230 students from the fourth, fifth, and sixth years of study (400–600 levels), representing the clinical phase of medical training. These years were chosen due to the heightened academic and clinical pressures students face during this period. The University’s College of Medicine is one of the major medical colleges established in Nigeria after independence and thus with its teaching hospital boasts of a robust training in the institution18. The fourth and fifth year medical students reside in the old site of the university while the sixth year medical students reside in the new campus, a rural area.
All clinical medical students who were willing to participate in the research were included in the study. However, Students who did not give consent to participate and those who were absent from school during the period of the study were excluded.
Sample size determination
The sample size was estimated using the formula for cross-sectional study involving a single population19.
n = Z>2 p (1 – p)/d2
where n is the sample size, Z is 1.96 at 95% confidence interval, P is the prevalence from a previous study (either as a percentage or fraction); 23.3% = 0.23319, d is the margin of error tolerated, usually 5% or 0.05 if prevalence is written as a fraction.
n = 1.962 × 0.233 (1–0.233)
0.052
n = 3.84 × 0.179 = 0.686/0.0025 = 274
0.0025
Minimum sample size (n) = 274.
To calculate the desired sample size (nƒ) when the population is less than 10 000.
Using the single population proportion formula: nƒ = ![]()
where nƒ is the desired sample size when the population is less than 10 000, n is the desired sample size when the population is more than 10 000, N is the estimate of the population size.![]()

An additional 10% of the minimum sample size was added to mitigate for nonresponse; adjusting for nonresponse
n1 = nƒ/ RR
where n1 is the adjusted sample size, nƒ is the minimum sample size calculated, RR is the expected response rate (usually expressed as a decimal); 0.9 n1 = 207/0.9 (90% response rate).
Sample size = 230.
Data collection method
A consecutive sampling technique was used to select students from each level of the clinical medical school. Hence, 79 questionnaires were distributed to 600 levels, while 76 and 75 questionnaires were distributed to 400 and 500 levels, respectively. This study focused on clinical medical students in their 400–600 levels because these years represent the clinical phase of medical training, which is associated with increased academic, clinical, and emotional stress. Students in these levels face the most intense periods of study, including patient interactions, clinical rotations, and professional examinations, which have been identified as major contributors to depression and mental health challenges. While earlier years may also have challenges, the focus of this study was on students experiencing the highest academic and clinical pressures.
Data was collected using a structured self-administered questionnaire. The data was collected every day from the March 31 to April 4, 2022 by the researchers. Respondents were given the questionnaire to fill after an informed verbal and written consent had been obtained. The questionnaires were administered at the hall of residence of the respondents.
The questionnaire contained three sections. Section A covered demographic characteristics such as age, sex, marital status, and religion. Section B covered the assessment of mood according to the Beck’s Depression Inventory (BDI) rating scale. Section C covered the possible trigger factors for depression among medical students.
BDI which was used to assess the prevalence and patterns of depression in this study, consists of 21 items which are answered on a multiple-choice scale. Each item attracts a score of 0–3 with higher figures indicating more severe symptoms.
The inventory divides the scores into 1–10 as “These ups and down are considered normal,” 11–16 as “mild mood disturbance,” 17–20 as “Borderline clinical disorder,” 21–30 as “Moderate,” 31–40 as “severe” and 40–63 as “Extreme” depression.
Data analysis
The data gathered from complete sets of questionnaires was collated, inputted, and analyzed using the IBM Statistical Product for Service Solutions version 25 (SPSS version 25).
Univariate and bivariate analyses were performed. The socio-demographic details of respondents were reported using descriptive statistics. Frequencies and percentages were used for categorical variables, while means and standard deviation was used for continuous variables. Cross tabulation was used to determine the relationship between dependent variables (including sociodemographic characteristics) and independent variables. Chi-square test was used for categorical variables while t-test was used for continuous data. Confidence interval was set at 95% and P-value of less than 0.05 was accepted as statistically significant.
Ethical consideration
Ethical clearance was obtained from the institutional review board. Informed consent was obtained from all participants before administering the questionnaire, having explained the purpose, risks, and benefits of the research.
This work has been reported in line with the STROCSS criteria20.
Results
A total of 230 questionnaires were administered to the selected participants in their fourth, fifth, and sixth years. All the questionnaires were analyzed.
The respondents were mainly in the age range 19–38 years for both male and female with a mean age of 23.87 ± 2.32 SD. Of the 230 participants, 63.9% were males, while 36.9% were females.
Their distribution according to level of study was 33.0%, 32.6%, and 34.3% for 400, 500, and 600 levels, respectively. Majority of the respondents were Christians (99.1%) and unmarried (98.3%).
As presented in Table 1, a large proportion of the respondents (83.0%) reside in the hostel. 13.5% reside off-campus, while 3.5% reside with parents at home. The marital status of the respondents’ parents revealed that 79.6% of the respondents have their parents still married and living together while 4% of them came from divorced family background. About 13.0% had lost one or both parents, while 3.0% were reared by separated parents.
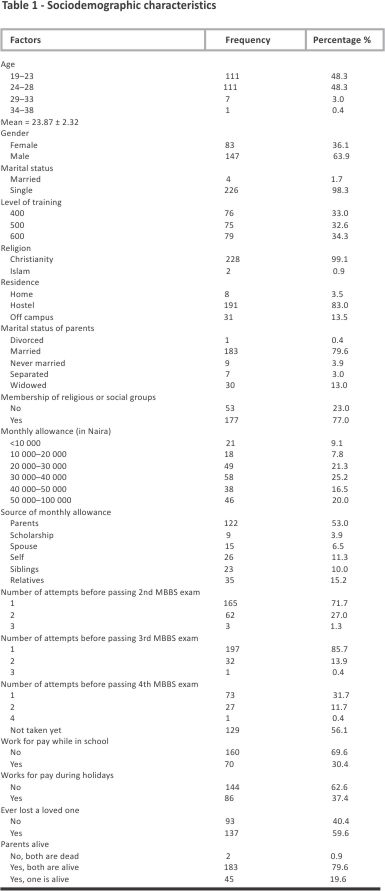
In 79.6% of cases, both parents were still alive, 19.6% had lost one parent, 0.9% had lost both parents (Table 1).
Table 2 shows that 26.5% of participants showed absolutely no symptom suggestive of depression, while 42.6% of patients had symptoms considered as normal using BDI.
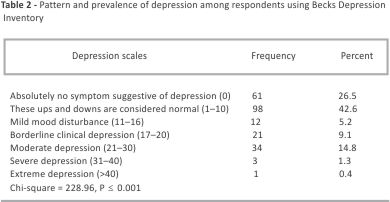
The prevalence of moderate depression among respondents was 14.8%, severe depression was 1.3% and extreme depression was 0.4%. Borderline clinical depression had a prevalence of 9.1%, while 5.2% of participants had mild mood disturbance with strong association (P < 0.001) between the depression scales of the participants.
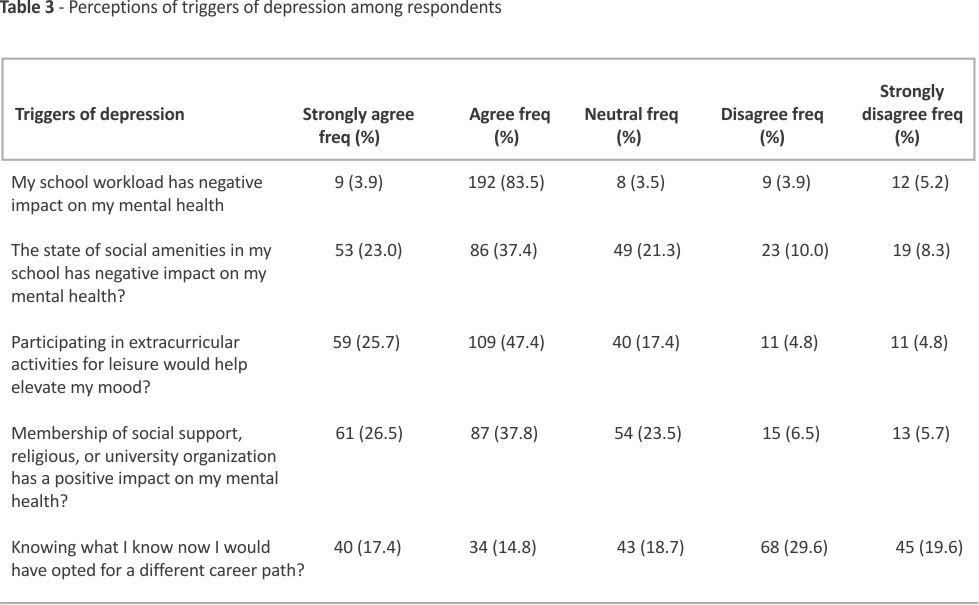
Table 3 shows that 92.5% of participants perceive school workload as having a negative impact on mental health. 60.4% perceive the state of school amenities as having a negative impact on health. For 64.3% of participants, membership of a social support, religious, or university organization has had a positive impact on their mental health. Additionally, 32.2% of students consider their choice of medicine as a factor in depression and would opt for a different career path if given the opportunity.
Participants who had monthly allowance of between 40 000 and 50 000 had the highest prevalence of borderline depression (28.6%), those with monthly allowance between 30 000 and 40 000 had highest prevalence of moderate depression. For severe depression, participants with monthly allowance of 20 000–30 000, 40 000–50 000, 50 000–100 000 had the same prevalence (33.3%) of severe depression (Table 4).
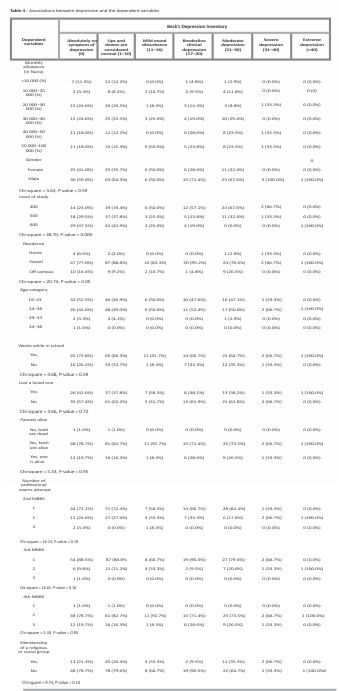
As shown in Table 4, the prevalence of borderline clinical depression was higher in males (71.4%) than in females (28.6%). Moderate depression had a higher prevalence also in males (67.6%) than in females (32.4%). Additionally, 100% of participants who had severe and moderate depression were male. However, these associations were not statistically significant.
Regarding level of study, 57.1% prevalence rate of borderline clinical depression in 400 level students, while students in 500 level and 600 level had prevalence rate of 23.8% and 19.0%, respectively. For moderate depression, there was prevalence rate of 67.6% and 32.4% for students in 400 level and 500 level respectively; 66.7% of severely depressed participants were in 400 level, while 33.3% were in 500 level. No participant in 600 level had moderate or severe depression. However, the only case of extreme depression was seen in a 600-level participant. The association between level of study and depression was highly significant (P < 0.001) (Table 4).
Table 4 also shows that there is no statistically significant relationship between depression and place of residence and age category of respondents.
Prevalence of borderline clinical depression, moderate, severe, and extreme depression for participants who resided in the hostel was 95.2%, 70.6%, 66.7%, and 100%, respectively. Those who resided off-campus had a prevalence of 4.8% and 26.5% for borderline and moderate depression, respectively, while 33.3% of participants residing at home had severe depression (Table 4).
There was no statistically significant relationship between depression and working while in school (P-value = 0.59).
Of participants with borderline clinical depression, moderate and severe depression 61.9%, 61.8%, and 66.7% had lost a loved one (P-value = 0.72), showing that the association with depression is not statistically significant.
Participants who had both parents alive had higher incidence of borderline, moderate, severe, and extreme depression, but this was not significant (P-value = 0.95) (Table 4).
Table 4 also shows that the prevalence of borderline clinical and moderate depression was higher for respondents who passed second MBBS on first attempt. For severe depression however, a higher prevalence rate (66.7%) was seen in respondents with two attempts at the second MBBS examination.
A higher prevalence of depression was shown for participants with only one attempt at the third MBBS examination. This association, though, is not statistically significant (P-value = 0.16).
Out of the participants with absolutely no depression, 78.7% belong to a religious or university support group. Of those with ups and downs considered as normal, 79.6% belonged also to a support group (Table 4).
Discussion
This study is on the prevalence and pattern of depression among clinical medical students in a medical school in southeastern. In recent years, the broad topic of clinical depression affecting the mental health of medical students has been identified and studied. However, there is a lack of knowledge about clinical depression regarding medical students in our university. The concept has received attention, including from the government, but the assumed pattern of presentations among medical students has not been the focus of attention. Therefore, this study goes the extra mile in assessing these patterns in detail taking note of the different variables that are pertinent to the population under study.
Gender differences in depression prevalence were observed, with males (63.9%) experiencing higher rates than females. However, this disparity may be influenced by the higher proportion of male respondents in the study. Interestingly, this contrasts with findings from a Babcock University study, where females exhibited higher depression rates21 but concurs with the findings in Saudi Arabia22. This variation highlights the need for further gender-specific mental health research in Nigerian medical schools.
It was noted that 5.2% of the participants had mild mood disturbance, prevalence of moderate depression was 14.8%, severe depression was 1.3% and extreme depression was 0.4%. Borderline clinical depression had a prevalence of 9.1%, giving a total prevalence of 30.8%.
The study showed varied prevalence of depression among different depression scales with moderate depression having the highest prevalence (14.8%) showing that one in seven medical students has depression. This is lower than that found in a study in Saudi Arabia that reported the prevalence of depression or depressive symptoms among medical students was 53.5%, with suicidal ideation at 11.1%22. Also, a study by Nezam et al to estimate the prevalence of depressive symptoms among professional course-seeking students showed a prevalence rate of 47.78%23. The discordance can be attributed to the difference in the data collection instrument used, study setting and medical school curriculum as they used Patient Health Questionaire-9 with a smaller population than ours. This underscores the significant mental health burden faced by medical students globally.
The prevalence of depression in our study (30.8%) aligns with global data, such as the 27.2% reported in a meta-analysis of depression among medical students worldwide12. However, studies from other Nigerian universities, such as the 17.4% prevalence found in Ebonyi State University, highlight variability in depression rates24. Differences in methodology, sampling, and the academic environment may explain these discrepancies. For example, our study exclusively targeted clinical students, who face more demanding work-loads and academic pressures than preclinical students, possibly accounting for the higher prevalence observed here. In contrast, studies like the one conducted at Babcock University, a private institution, reported higher rates of depression among females25, with a lower overall prevalence, possibly due to differences in academic structures, support systems, and socioeconomic factors. The presence of more supportive infrastructures in private institutions, such as smaller class sizes and better facilities, may reduce stressors that are more prevalent in public universities like ours. It was also noted that 26.5% of participants showed absolutely no symptoms suggestive of depression while 42% of patients had symptoms considered as normal using BDI. This is in contrast to the result of a cross-sectional study carried out on all matriculated medical students of Ebonyi State University Abakaliki, Nigeria which showed the prevalence of depression to be 17.4%24. However, this could be attributed to the difference in sample population used as this study recruited only clinical medical students. A study amongst medical students in Babcock University, Ogun State Nigeria showed moderate depression and severe depression had prevalence rates of 1.0% and 9.0%, respectively25. This also could be due to differences in study location and population used as the school we studied is a public school while the study in Ogun utilized a private medical school hence there might be significant changes in the training modalities employed.
On the potential triggers of depression, it was noted that financial constraints had no positive correlation with depression as 83% of the participants had an income of greater than 20 000 naira. Notably, participants who had monthly allowance of 40–50 000 naira had the highest incidence of borderline depression (28.6%) and those with monthly allowance between 30 and 40 000 naira had the highest prevalence of moderate depression. This is supported by the studies by Zafar et al26, Obilade et al27, and Chukwuneke et al28. There was also no positive correlation between depression and re-sitting medical professional exams as 85.7% of the participants passed third MBBS (pathology and pharmacology) at the first attempt. For severe depression however, a higher prevalence rate (66.7%) was seen in respondents with two attempts in the second MBBS (preclinical) examination. Academic workload has been consistently identified as a primary trigger for depression among medical students. In our study, a significant proportion of students cited academic pressures as a major contributor to their depressive symptoms. This is corroborated by findings from other Nigerian universities, where academic stress was a prevalent factor among depressed students29. About 60.4% perceived the state of school amenities as having a negative impact on health. This was corroborated by a study by Elsawy et al30 where students that noted poor environment for studying had higher prevalence of depression compared to others.
For 64.3% of participants, membership of social support, religious, or university organization has had a positive impact on their mental health. This is in line with the study focusing on nursing and medical students in Muslim-majority contexts which found that higher levels of religiosity were associated with lower levels of depression and stress31. This suggests that personal faith may serve as a coping mechanism against psychological distress in these populations. Additionally, 32.2% of students consider their choice of medicine as a factor in depression and would opt for a different career path if given the opportunity. This is in agreement to previous studies that gave similar result25,26,29,31. The reason for this, we believe is due to the workload and level of stress,25 as well as reduced passion for the profession which might be indirectly influenced by the impact of the nation’s economy on the profitability of professions32–34.
About two-third of participants see participating in extracurricular activities as a means to elevate mood. A 2018 study to determine the level of stress, depression, and anxiety in the College of Medicine of Lagos State University students determined that of 240 respondents with 25 years as the mean age from the second to the sixth year, 6.3% of them experienced depressive symptoms. This rate is lower than is found in other studies34,35. The probable reason cited was the fact that the medical hostel was very close to the medical college, thus, students did not have to travel far to get to school, that most of the participants come from affluent families and likely received adequate moral and financial support from their parents34,35. This though is at variance with other published evidence that indicates that financial problems and travelling between medical school and home were factors that caused psychological distress for students35.
The study additionally found that 61.6% of the students experienced symptoms of stress – a major etiologic factor for depression. Of participants with absolutely no depression, 78.7% belong to a religious or university support group. Of those with ups and downs considered as normal, 79.6% belonged also to a support group. This shows the need for social and peer, and pressure groups which can help to improve the mood of her members29–32.
Also, in Nigeria, mental illness, including depression, is heavily stigmatized. Cultural beliefs often frame mental health conditions as personal failings or spiritual issues, leading many to seek spiritual interventions rather than professional medical care. For instance, depression might be seen as a result of supernatural forces or spiritual attacks, which discourages individuals from accessing psychiatric treatment35,36. This deep-rooted stigma contributes to the underreporting of symptoms and delays in seeking help. This may have affected the lower prevalence seen in other studies compared to ours.
Moreover, religious and traditional healing systems are widely preferred, as many believe that prayer or spiritual rituals can resolve mental health issues. While such systems can offer emotional support, they often impede early medical intervention. This cultural backdrop, combined with limited awareness of mental health issues, presents significant barriers to improving mental health outcomes. Efforts to promote mental health literacy, reduce stigma, and integrate culturally appropriate interventions remain crucial for addressing these challenges36,37.
The findings of this study reflect the influence of Nigeria’s socioeconomic and cultural context on the mental health of medical students. Financial insecurity, stemming from widespread poverty, alongside poor infrastructure and limited amenities in underfunded public universities, contributes significantly to stress levels. Additionally, the high academic pressures in these institutions, combined with societal expectations for excellence, further exacerbate mental health challenges. Cultural stigma surrounding mental illness discourages students from seeking professional help, with many relying on religious or traditional support systems instead. Weak institutional support, social isolation, and frequent university strikes add to the burden, creating an environment where depressive symptoms are likely to thrive. The depression prevalence of 30.8% observed in this study aligns with global averages but exceeds some local reports, underscoring the compounded impact of economic, cultural, and systemic factors on the mental health of clinical medical students in Nigeria38,39.
Limitations
This study has several limitations. First, it did not account for participants’ personal or family history of depression, which is known risk factors for developing depression. Second, the use of self-administered questionnaires, while practical, may introduce recall or response bias. Also, the cross-sectional design limits our ability to draw conclusions about causality. Longitudinal studies would be better suited to examine how depression evolves throughout medical training. Additionally, while the BDI is traditionally used to assess the severity of depression in clinical settings, it has also been employed as a tool for assessing depressive symptoms in nonclinical populations, including medical students. In this study, the BDI was used to capture the severity of depressive symptoms across a spectrum of normal to severe depression. However, it is important to note that no clinical diagnosis was made, as formal psychiatric interviews were not conducted. The BDI allowed us to quantify the presence and severity of depressive symptoms, but this study does not confirm clinical diagnoses.
Additionally, the study’s inability to conduct inferential analysis is noted as limitations. Therefore, future research could benefit from longitudinal designs and advanced statistical methods.
Recommendations
Based on the findings from this study, several interventions are recommended to address the high prevalence of depression among clinical medical students in the University of Nigeria. These recommendations aim to enhance mental health awareness, provide better support systems, and improve the overall academic environment to reduce mental health burdens.
To address the high prevalence of depression among medical students, institutions should establish student-friendly counseling units that provide confidential support and stress management training. Mental health education should be integrated into medical curricula, equipping students with coping strategies for academic and professional challenges.
Universities should promote peer-support networks and extra -curricular activities to enhance social engagement and reduce isolation. Membership in student organizations, religious groups, and volunteer programs should be encouraged, as they have been shown to positively impact mental well-being.
Medical schools must restructure academic workloads to reduce undue pressure. This includes revising assessment methods by incorporating continuous assessments instead of solely relying on high-stakes exams. Faculty should receive mental health awareness training to better support students showing signs of distress.
Additionally, institutional policies should ensure adequate social amenities, as poor living conditions contribute significantly to stress. Investment in hostel upgrades, improved recreational facilities, and accessible healthcare services is essential.
Nationwide surveys on medical student depression should be conducted to inform evidence-based interventions and policies. A multi-sectoral approach involving universities, mental health organizations, and government bodies is necessary to address systemic issues affecting student well-being.
Prioritizing mental health support in medical education will foster resilience, improve academic performance, and ultimately enhance future healthcare professionals’ well-being and efficiency.
Conclusion
The high prevalence of depression among medical students under- scores the urgent need for targeted interventions. Factors such as academic overload, inadequate social amenities, and lack of institutional mental health support significantly contribute to psychological distress. However, peer support networks, extracurricular engagement, and improved mental health services have demonstrated positive impacts.
A collaborative effort involving universities, policymakers, and mental health organizations is crucial in developing structured interventions that promote resilience and well-being among medical students.
Ethical approval
Not applicable.
Consent
Not applicable.
Sources of funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not for- profit sectors.
Author contributions
O.B.C., O.P.U., O.C.F., O.C.J., and O.O.V. conceived, designed the study, and conducted the research. O.W.O., O.C.A., and I.W.C. provided research materials, collected and organized data. I.D.A. and O.C.P. analyzed and interpreted data. O.B.C., O.P.U., O.C.F., O.C.J., O.O.V., U.C.V., T.O.S., U.C.C., N.U. wrote initial and final draft of article, I.S.N., N.P.C., O.N., O.E.O. provided logistic support. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
Conflicts of interest disclosure
We have no conflict of interest to declare.
Guarantor
Promise Udohchukwu.
Provenance and peer review
Not applicable.
Data availability statement
Not applicable.
References
[1]. WHO. Depression. Retrieved from https://www.who.int/news-room/fact-sheets/detail/ depression
[2].Felix T. What is Depression. Retrieved from https://www. psychiatry.org/patients-families/ depression/what-is-depression
[3]. Paykel ES. Basic concepts of depression. Dialogues Clin Neurosci 2008;10:279.
[4]. WHO. (2017). Depression and Other Common Mental Disorders, Global Health Estimates.
[5]. WHO. (2012). Depression: A Global Public Health Concern.
[6]. Yussof M, Baba A. Prevalence and associated factors of stress, anxiety and depression among prospective medical students. Asian J Psychiatr 2013;6:128–33.
[7]. Waqas A, Khan S, Sharif W, et al. Association of academic stress with sleeping difficulties in medical students of a Pakistani medical school: a cross sectional survey. PeerJ 2015;3:e840.
[8]. Styles WM. Stress in under- graduate medical education: ‘the mask of relaxed brilliance.’ Br J Gen Pract 1993;43:46–47.
[9]. Lloyd C, Gartrell NK. Psychiatric symptoms in medical students. Compr Psychiatry 1984;25:552– 65.
[10]. Rosal MC, Ockene IS, Ockene JK, et al. A longitudinal study of students’ depression at one medical school. Acad Med 1997;72:542– 46.
[11].Yusoff MSB, Mat Pa MN, Esa AR, et al. Mental health of medical students before and during medical education: a prospective study. J Taibah Univ Med Sci 2013;8:86–92.
[12].Rotenstein LS, Ramos MA, Torre M, et al. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: a systematic review and meta-analysis. Jama 2016;316:2214–36.
[13]. Onyishi M, Talukdar D, Sanchez R, et al. Prevalence of clinical depression among medical students and medical professionals: a systematic review study. Arch Med 2016;8(6).
[14]. Kebede MA, Anbessie B, Ayano G. Prevalence and predictors of depression and anxiety among medical students in Addis Ababa, Ethiopia. Int J Ment Health Syst 2019;13:1–8.
[15].Tjia J, Givens JL, Shea JA. Factors associated with undertreatment of medical student depression. J Am Coll Health 2005;53:219–24.
[16].Dyrbye LN, Thomas MR, Massie FS, et al. Burnout and suicidal ideation among US medical students. Ann Intern Med 2008;149:334– 41.
[17].Dyrbye LN, Thomas MR, Shanafelt TD. Systematic review of depression, anxiety, and other indicators of psychological distress among US and Canadian medical students. Acad Med 2006;81:354–73.
[18].Malu AO. Universities and medical education in Nigeria. Niger Med J 2010;51(2).
[19]. Sharma SK, Mudgal SK, Thakur K, et al. How to calculate sample size for observational and experimental nursing research studies. Natl J Physiol Pharm Pharmacol 2020;1 0:1–8.
[20].Mathew G, Agha R. For the STROCSS Group. STROCSS 2021: strengthening the Reporting of cohort, cross-sectional and case-control studies in Surgery. Int J Surg 2021;96:106 165.
[21].Coker AO, Coker OO, Sanni D. Socio demographic correlates and symptoms of depression, anxiety and stress among a sample of Nigerian medical students. Nigerian J Basic Clin Sci 2018;15:58–62.
[22].Alshahrani AM, Al-Shahrani MS, Miskeen E, et al. Prevalence of depressive symptoms and its correlates among male medical students at the University of Bisha, Saudi Arabia. Healthcare 2024;12:640.
[23].Nezam S, Golwara AK, Jha PC, et al. Comparison of prevalence of depression among medical, dental, and engineering students in Patna using Beck’s Depression Inventory II: a cross-sectional study. J Family Med Prim Care 2020;9:3005–09.
[24].Tamunosiki C, Chinawa J, Aniwada E, et al. Determinants of depression among medical students in two medical schools from South East Nigeria: a screening test. The Ann Niger Med 2017;11:27–31.
[25].Dike-Israel N, Akinboye D. Prevalence and comorbidity of depression and anxiety among medical students in Babcock University, Ogun State, Nigeria. Asian J Med Health 2021;19:46– 55.
[26].Zafar M, Rizvi SB, Sheikh L, et al. Comparative analysis of depression and its associated risk factors among public and private medical schools students in Karachi, Pakistan: a multicenter study. Saudi J Health Sci 2017;6:1–7.
[27].Obilade TT, Koleoso PO, Nwenendah-Mpi EW. An investigative study on the causes of depression and the coping strategies among clinical medical students in private universities in North Central Nigeria. BMC Psychiatry 2024;24:10.
[28].Chukwuneke G, Udogu I, Luwasi N, et al. A Comparative study of the prevalence of depression among clinical medical students in a private and public university in Plateau State, North Central Nigeria. Afr J Res Med Health Sci 2024;2:39–42.
[29].Oluoha RU, Offiong AA, Okafor PN, et al. Prevalence and predictors of depression among medical students of Imo State University, Owerri, South Eastern Nigeria. Int J Trop Dis Health 2023;44:31–40.
[30]. Elsawy WI, Sherif AA, Attia MS, et al. Depression among medical students in Alexandria, Egypt. Afr Health Sci 2020;20:1416–25.
[31]. Rammouz I, Lahlou L, Salehddine Z, et al. Religiosity, stress, and depressive symptoms among nursing and medical students during the middle stage of the COVID-19 pandemic: a cross-sectional study in Morocco. Front Psychiatry 2023;14:1123356.
[32].Lou Q, Hairong H, Yang J, et al. Changes in global burden of depression from 1990 to 2017: findings from the Global Burden of Disease Study. J Psychiatr Res 2020;126:134–40.
[33].Record R, Mohiddin A. An economic perspective on Malawi’s medical” brain drain”. Glob Health 2006;2:1–8.
[34].Budhathoki SS, Zwanikken PA, Pokharel PK, et al. Factors influencing medical students’ motivation to practise in rural areas in low-income and middle-income countries: a systematic review. BMJ Open 2017;7:e0135 01.
[35]. Evans-Lacko S, Agullar-Gaxiolla S, AL-Hamzawi A, et al. Socio-economic variations in the mental health treatment gap for people with anxiety, mood substance use disorder: results from the WHO World Mental Health (WMH) surveys. Psychol Med 2018;48:1560–71.
[36].Abba Aji M, Galea S Mind the widening gap: a trauma-driven mental health crisis in Nigeria. BMJ Glob Health Blog. 2023. https://blogs.bmj.com/bmjgh/2024/05/26/mind-the-widening-gap-a-trauma-driven-mental-health-crisis-in-nigeria.
[37].Mental Health in Nigeria: A Comprehensive Overview. Man and Microbes. 2023. Available from: https://manandmicrobes.com/mental-health-in-nigeria
[38].Fadele KP, Igwe SC, Toluwalogo NO, et al. Mental health challenges in Nigeria: bridging the gap between demand and resources. Camb Prism: Glob Ment Health 2024;11:e29.
[39].Nweke SC, Ewelike SC, Okon II, et al. Problems and critical reforms in mental health care: an examination of Nigeria’s situation. IJS Global Health 2024;7:e00486.
Credit: Okereke, Promise Udohchukwu BDSa,b,c,*; Obiora, Benjamin Chidum MBBSd; Obu, Franklin Chibueze MBBSd; Ochi, Chizoba Judith MBBSd; Odigidawu, Onyebuchi Victor MBBSd; Okereke, Obumneme Wisdom BDSb,e; Umeh, Chukwuemeka Victor MBBSf; Tola, Olalekan Simeon MBBSg; Ibekwe, Solomon Nnayelugo BDSa,h; Nnaji, Uche MBBSi; Ifedibar, Chisom Wisdom MBBSj; Uche, Collins BDSa,k; Nnegboh, Philip Chukwunonso MBBSd; Ogbu, Andrew Chukwuemeka MBBSl; Ogamba, Nzubechukwu MBBSd; Ogunlana, Olaoluwaposi Emmanuel MBBSm. Prevalence and patterns of depression among clinical medical students in a major medical college in southeast Nigeria: a cross-sectional study. International Journal of Surgery: Global Health 8(3):e00564, May 2025. | DOI: 10.1097/GH9.00000 00000000564