

Deepika Laddu, PhD, FAHA, Chair, Ian J. Neeland, MD, FAHA, Vice Chair, Mercedes Carnethon, PhD, FAHA, Fatima C. Stanford, MD, MPH, MPA, MBA, FAHA, Morgana Mongraw-Chaffin, PhD, FAHA, Bethany Barone Gibbs, PhD, FAHA, Chiadi E. Ndumele, MD, PhD, FAHA, Chris T. Longenecker, MD, FAHA, Misook L. Chung, PhD, RN, FAHA, and Goutham Rao, MD, FAHA on behalf of the American Heart Association Obesity Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Epidemiology and Prevention; Council on Clinical Cardiology; Council on Hypertension; Council on the Kidney in Cardiovascular Disease; and Council on Cardiovascular and Stroke Nursing
Abstract
Obesity is a recognized public health epidemic with a prevalence that continues to increase dramatically in nearly all populations, impeding progress in reducing incidence rates of cardiovascular disease. Over the past decade, obesity science has evolved to improve knowledge of its multifactorial causes, identifying important biological causes and sociological determinants of obesity. Treatments for obesity have also continued to develop, with more evidence-based programs for lifestyle modification, new pharmaco-therapies, and robust data to support bariatric surgery. Despite these advancements, there continues to be a substantial gap between the scientific evidence and the implementation of research into clinical practice for effective obesity management. Addressing barriers to obesity science implementation requires adopting feasible methodologies and targeting multiple levels (eg, clinician, community, system, policy) to facilitate the delivery of obesity-targeted therapies and maximize the effectiveness of guideline-driven care to at-need patient populations. This scientific statement (1) describes strategies shown to be effective or promising for enhancing the translation and clinical application of obesity-based research; (2) identifies key gaps in the implementation of obesity science into clinical practice; and (3) provides guidance and resources for health care professionals, health care systems, and other stakeholders to promote broader implementation and uptake of obesity science for improved population-level obesity management. In addition, advances in implementation science that hold promise to bridge the know-how gap in obesity prevention and treatment are discussed. Last, this scientific statement highlights implications for health research policy and future research to improve patient care models and optimize the delivery and sustainability of equitable obesity-related care.
The prevalence of obesity in the United States and globally has been escalating for decades, with recent estimates that >40% of US adults are living with obesity.1,2 The continued rise in obesity has inevitably slowed the decline in rates of cardiovascular disease (CVD) despite improvements in other population risk factors.3 Moreover, forecasted trends in global obesity prevalence underscore the significant impact that obesity will continue to have on CVD incidence, especially among people of underrepresented races and ethnicities.4–6 Over the past decade, significant progress made in obesity science has contributed to the discovery of knowledge cutting across the domains of basic, translational, and biobehavioral science; epidemiology; and clinical studies/trials. Treatment of obesity also continues to evolve, with more empirical evidence supporting the efficacy of lifestyle modification programs, new pharmacotherapies, and robust outcomes data for bariatric surgery.
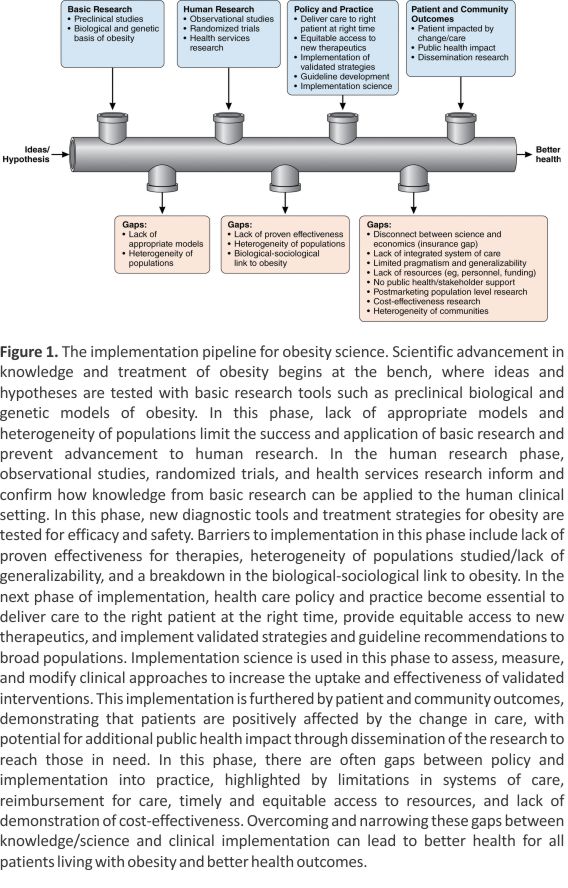
Despite the ubiquity of these advancements, the effective implementation of obesity science into routine clinical practice for the prevention and treatment of obesity remains sub-optimal. There are major gaps between our knowledge of the science of obesity and the clinical implementation of that science for ideal patient care. The lack of sufficient implementation exemplifies important gaps that exist between our biological and sociological understanding of obesity, interventions that target obesity (eg, lifestyle, pharmacological, and surgical), and the application of evidence-based research into clinical practice for improved management of obesity.7–9 These gaps are sustained by structural, societal, and cultural barriers that are pervasive in real-world clinical practice and require a redoubling of efforts and alternative strategies for resolution and advancement. Therefore, prioritizing the implementation of obesity science will be instrumental in informing evidence-based practice and consequently guiding the delivery and maintenance of contextually appropriate care to diverse, under-represented populations with obesity. 10,11 Bridging the gap in obesity implementation science requires a multitargeted approach that addresses long-standing implementation challenges across various levels (eg, clinician, community, system, policy) and applies effective implementation strategies based on core frameworks11,12 to advance the integration of novel, empirically supported obesity science into routine clinical care (Figure 1).
METHODS FOR SUCCESSFUL IMPLEMENTATION OF OBESITY SCIENCE INTO CLINICAL PRACTICE
The successful implementation of obesity science into clinical practice requires a methodological framework that moves scientific knowledge from bench to bedside and addresses gaps in the implementation pipeline. Obesity science is well established, and emerging therapeutic options based on scientific discoveries have become increasingly prevalent in the past several years. Education on the complex origins and clinical consequences of obesity, a framework for the successful delivery of obesity care, and health policy interventions to enhance the provision of obesity care are examples of implementation priorities that are essential to the success of obesity science.
To address the growing obesity epidemic and successfully implement obesity science, healthcare professionals must first be equipped with the proper knowledge and implementation skills. Yet, numerous studies have demonstrated that obesity education is lacking. For example, although the American Board of Medical Specialties certification examinations influence medical knowledge and practice for physicians throughout the United States, only 25% of the 24 general certification content outlines (ie, preparatory material for examinations) mention obesity. This gap indicates a need for translating the complexity of obesity science into practice with an increased emphasis on the diagnosis, prevention, and treatment of obesity.13 In a comprehensive international systematic review on obesity education across varying levels of medical training, Mastrocola and colleagues14 determined that there is a paucity of obesity education programs for medical students, residents, and fellow physicians in training programs worldwide despite high obesity prevalence. Still, they note that these programs often improve outcomes when administered.
One increasingly successful method for improving healthcare professional education and subsequent implementation is the certification program in obesity medicine offered by the American Board of Obesity Medicine (ABOM). Studies show that physicians certified in obesity medicine tend to deliver more effective evidence-based care, such as lifestyle and behavioral counselling, pharmacotherapy, and care for patients who undergo metabolic and bariatric surgery.15 In a cross-sectional analysis of the ABOM-certified physicians, certified physicians’ practices were likely to be concordant with published guidelines, including the American College of Cardiology/American Heart Association/The Obesity Society, American Association of Clinical Endocrinologists/American College of Endocrinology, and Obesity Medicine Association guidelines. However, although healthcare practitioners may be confident that ABOM-certified physicians will deliver evidence-based care, access to these physicians is often unavailable because of the high prevalence of obesity and the relative shortage of certified professionals. Although all states in the United States have at least 1 ABOM-certified adult physician, there are geographic disparities in physician availability relative to obesity prevalence, leading to widened healthcare disparities. This is even more pronounced in the pediatric population, with fewer ABOM-certified physicians.
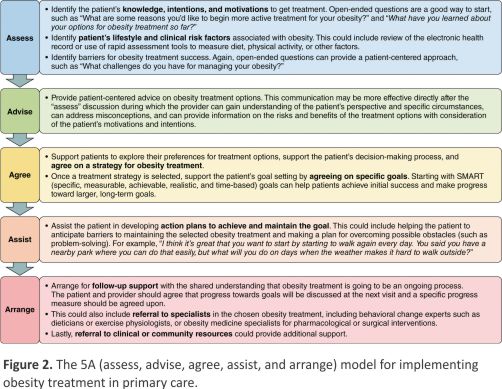
The next step in implementation requires a framework for successfully delivering obesity medicine care. The Society for Behavioral Medicine has an evidence-based model for primary care obesity management based on the 5As counseling framework (assess, advise, agree, assist, and arrange),16 of which can be used to promote the implementation of obesity treatments in clinical practice settings (Figure 2). Two recent American Heart Association statements provide a comprehensive summary of how to implement the 5A model for health behavior change in primary care and community-based settings for CVD prevention and risk management.17,18 There is a particular focus on guiding primary healthcare professional efforts to offer or refer patients for behavioral counseling beyond what can be done during the brief, episodic office visits.17 Best-practice approaches for enhancing the adoption and implementation of behavior change programs in clinical or community-based health care settings, including the use of team-based care, reimbursement and referral models, and practical national resources, are described in detail.17,19 Although more studies are needed on the effectiveness of healthcare professional–delivered behavior counseling interventions on the maintenance of behavioral outcomes, promoting a healthy lifestyle and assisting patients in achieving health behavior goals presents a feasible strategy that healthcare professionals in clinical and community-linked settings can use to proactively maximize impact on obesity care and reduce the burden of subsequent CVD risk at every visit.18 It is important to note that building solid, sustainable clinic-community linkages is necessary to facilitate the implementation of obesity/weight management programs. Indeed, increasing clinician education and self-efficacy in obesity science, along with the workforce of specialized ABOM-certified diplomates, while building straightforward evidence-based treatment workflows with expanded and adequate clinician reimbursement, also appears to be the logical next step to the successful implementation of obesity science into clinical practice.20
Health policy interventions that can enhance the provision of obesity care are emerging globally. One example is Life’s Essential 8, the key measures for improving and maintaining cardiovascular health as defined by the American Heart Association.22 The goal of Life’s Essential 8 is to link science to implementation. Many of the Life’s Essential 8 health behaviors and habits affect body weight, and the Life’s Essential 8 advisory contains important methods for implementing cardiovascular health assessment and longitudinal monitoring, as well as potential data sources and tools to promote widespread adoption in policy, public health, clinical, institutional, and community settings.
IDENTIFYING GAPS IN OBESITY SCIENCE: CLINICIAN KNOWLEDGE, COMFORT, AND SENSITIVITY; PATIENT AVOIDANCE; CONNECTION TO RESOURCES; AND COST-EFFECTIVENESS
A critical gap in implementing obesity science into practice is the central focus on ascertaining a particular body weight. Obesity, as traditionally defined by body mass index (BMI), is remarkably heterogeneous, and the use of the BMI alone leads to confusion about when and how to initiate targeted obesity interventions. It is well known that BMI cannot distinguish between lean and fat mass and that it fails to discriminate between adipose tissue depots in different anatomic regions. For example, a BMI-centric approach has spawned a debate about metabolically healthy obesity, referring to populations with lower cardiovascular risk due to lower visceral abdominal adiposity and higher levels of cardiorespiratory fitness despite an elevated BMI.23,24 Moreover, the debate about the potential dangers of weight loss and the concept of the obesity paradox—whereby patients with symptomatic CVD (eg, heart failure) who maintain higher body weight (overweight or class I obesity) experience improved survival—has led to controversies, particularly in cardiovascular medicine, and skepticism of the merits in prescribing weight loss interventions to patients with existing cardiac conditions.24,25 These weight-centric approaches to obesity management, rather than a focus on obesity-related complications and adverse health outcomes, can be confusing and may discourage some clinicians from even considering obesity management interventions. Therefore, it is clear that we need better tools to assess the degree of obesity and its relationship to associated health risks. Furthermore, overreliance on BMI may paradoxically hinder efforts by clinicians in many settings to address obesity. The net effect is that the vast majority of patients whom clinicians encounter may benefit from weight management. Therefore, BMI adds little useful information for most clinicians in terms of how to prioritize care for obesity based on the risk of obesity-related conditions. There is evidence that waist circumference may be useful in this regard; however, implementing routine measurements and actionable steps to address waist circumference in the context of BMI remains a challenge in clinical practice.
Implementation Gaps in Lifestyle Interventions
In a recent study, few healthcare practitioners (16%) could identify evidence-based lifestyle treatments for obesity, and there was a high level of heterogeneity by practice type.26 This included low levels of working knowledge about diet and nutrition specialists (i.e., when to refer and identification of barriers to specialist referral), intensive behavioral therapy, and physical activity. This gap in recognition may help explain the low rates of referrals to clinical weight management programs and other weight-reduction systems for those who are eligible. Further barriers include a lack of clinician comfort in initiating and conducting discussions about obesity with patients; hesitancy to reduce trust or offend patients who may be seen, incorrectly or not, as wanting to avoid these interactions; assumptions about patient interest in weight management strategies and access to them; and structural issues such as poor coverage or low levels of reimbursement for obesity-related care.
Not surprisingly, 23% of patients never speak to a clinician about their weight or lifestyle interventions for weight management. When discussions did occur, almost 60% of respondents reported that clinicians never asked for permission before discussing sensitive issues related to obesity, and only about half (52%) thought that their clinician understood the challenges of being overweight or obese.27 Thirty percent of respondents reported that their clinician did not discuss resources for weight management. Last, >15% of patients reported not seeking care to avoid being weighed or having discussions about weight, with a higher prevalence for those with more severe obesity.27 This is a major gap in implementation, given that there is clear evidence that intensive lifestyle therapy is considerably more effective than brief advice, and general educational information is provided far more often by physicians than connection or referral to classes, programs, or tangible resources for lifestyle change.19,27
Clinicians need to adopt effective and sensitive ways to initiate discussions about weight. As part of a 2017 roundtable workshop,21, Rao describes the “opening the door” approach to initiating discussions, which seeks permission to initiate discussions in a direct but sensitive way that allows the engagement of patients in further obesity-related discussions. One way to open the door is the following21: “I am concerned about your weight. It puts you at risk for several conditions such as diabetes. Is this something that concerns you as well? Is this something you would like to discuss and work on together?”
Alternatively, patients can be empowered to ask their clinicians about weight. Patient empowerment is an important, emerging concept in the engagement and delivery of health care.28 Patients can be encouraged to ask questions about a wide range of issues of importance to them related to their care.29 Prompts (sent, for example, by an electronic patient portal) such as “Don’t forget to ask your doctor about your weight” or encouraging the question “I’m concerned about my weight and would like your help in achieving and maintaining a healthy weight” are easy ways for patients and clinicians to begin discussions. Many of the barriers to receiving obesity care are exacerbated by socioeconomic and racial or ethnic inequities. Despite a greater interest in weight management conversations and opportunities,27 underrepresented racial and ethnic groups and those with public insurance are less likely to be referred to weight management programs or have them covered by insurance.30 Furthermore, there is a significant contribution of psychiatric/psychological factors in terms of both contributing to obesity and creating barriers to engaging in appropriate therapies that are not adequately addressed in current care models.
Implementation Gaps in Pharmacotherapies for Treating Obesity
Newer pharmacotherapies for obesity treatment demonstrate impressive effectiveness in real-world settings that approximate their efficacy in clinical trials. The 2 pharmacotherapies approved most recently by the US Food and Drug Administration (FDA) for long-term weight management are high-dose semaglutide and tirzepatide, which are both associated with an average weight loss of >10% at 6 months in clinical environments, greater than weight loss achieved from other FDA-approved antiobesity medications (AOMs).31,31a However, obesity pharmacotherapies continue to be dramatically underprescribed. Although >50% of adults meet the eligibility criteria for obesity pharmacotherapies, a striking minority of adults trying to lose weight are receiving these agents.32,33 These prescribing patterns for obesity pharmacotherapies stand in stark contrast to those for diabetes and hypertension, conditions that are common consequences of obesity.
The reasons for the low use rates of obesity pharmacotherapies are likely related principally to (1) knowledge gaps among clinicians, (2) concerns about the safety of obesity pharmacotherapies, and (3) perhaps most importantly, coverage limitations. A survey of health professionals demonstrated that only 15% of clinicians were familiar with the guideline-directed indications for prescribing obesity pharmacotherapies.26 A report from the Government Accountability Office identified limited clinician education and experience related to the provision of obesity pharmacotherapies as a critical barrier to the appropriate use of these medications.33 The low use of obesity pharmacotherapies is also linked to widespread concerns about their potential harms. These concerns likely reflect a legacy effect of the relatively high side effects of older sympathomimetic and combination obesity medications relative to those seen with newer glucagon-like peptide-1 receptor agonists and dual glucagon-like peptide-1 and glucose-dependent insulinotropic polypeptide receptor agonist agents. A 2018 statement from the US Preventive Services Task Force describing the potential harm of obesity pharmacotherapies compared with lifestyle modification may have a powerful influence on clinicians.
Perceptions about the safety of obesity pharmacotherapies.34 Perhaps the most significant barrier to the greater use of obesity pharmacotherapies is limited coverage and high out-of-pocket costs for these medications. A 2016 analysis of health insurance plans within the marketplace exchanges demonstrated that only 11% of the plans had some coverage for obesity pharmacotherapies.35 Additionally, although only 7 state Medicaid plans provided coverage for obesity pharmacotherapies, historically, Medicare Part D has explicitly excluded them. Given the high cost of these agents, these coverage limitations have contributed significantly to the undertreatment of excess weight, particularly in high-risk, underrepresented, and historically excluded populations with the highest burden of obesity and its associated comorbidities.
The recent approval by the FDA to expand the indication of the AOM semaglutide to reduce the risk of cardiovascular death, heart attack, and stroke in adults with CVD and either obesity or overweight based on the results of the SELECT (Semaglutide Effects on Heart Disease and Stroke in Patients With Overweight or Obesity) trial35a is the first step in a potentially major transformation shifting the coverage conversation away from obesity treatment for the goal of weight management to obesity treatment to reduce the risk of resulting adverse clinical consequences. Building on this shift, the Centers for Medicare & Medicaid Services recently issued guidance to Medicare Part D plans stating that AOMs that receive FDA approval for an additional medically accepted indication (eg, CVD) can be considered a Part D drug for that specific use. State Medicaid programs for low-income populations, who are disproportionately affected by obesity and CVD, will also be required to cover FDA-approved AOMs for this same population. However, states may still require step therapy with other medications or treatments before authorization, posing potential delays in access. This news marks transformational progress in policy toward expanding access to AOMs for high-risk, high-need patients for the prevention of adverse cardiovascular events. Nevertheless, ongoing challenges remain, as supplies of glucagon-like peptide-1 agonists, in particular, have been scarce, further limiting their use.
Implementation Gaps in Metabolic and Bariatric Surgery
Bariatric surgery has long been considered the last-line therapy for severe obesity that cannot be managed through lifestyle changes or pharmacotherapies alone. Since bariatric surgery was introduced in the 1950s, the procedures have become safer and more effective.36 In an umbrella review of meta-analyses, patients who underwent bariatric surgery had lower risks for incident CVD, multiple other obesity-associated conditions (eg, type 2 diabetes, hypertension), and adverse pregnancy outcomes, including gestational hypertension and diabetes.37 Among patients with preexisting type 2 diabetes or CVD who underwent bariatric surgery, glycemic parameters and measures of cardiac structure and function improved.38,39 As surgical expertise has grown, eligibility has expanded to include adults with type 2 diabetes and a BMI between 30 and 35 kg/m2,40 as well as adolescents with severe obesity and at least 1 major comorbidity.41 These safety advances and health benefits offer clinicians and patients another option to treat severe obesity.
The critical challenge facing the field is ensuring that the populations with the greatest needs can access bariatric surgery. A significant barrier to the implementation of bariatric surgery, despite established disparities in the prevalence of severe obesity, is that adolescents and adults who identify as Black or Hispanic/Latino and those who have fewer social and economic resources are far less likely to undergo surgery.40,42,43 Although structural factors that unfairly limit access to surgery account for some of the inequities, additional reasons include the perception and reality that the social supports needed for surgery to be successful are absent in underresourced populations with the greatest needs. Another gap in implementation may relate to the complexity of bariatric surgery that requires patients to have high levels of health literacy to enact the behavioral modifications necessary for favorable long-term (ie, 2-4 years) weight loss and maintenance.44 Furthermore, widespread availability of high-volume centers is lacking, and as with any procedure, higher bariatric surgical volumes are associated with better outcomes.45 High-volume bariatric surgery centers are more likely to be in major metropolitan areas and academic medical centers, which are the places that are less likely to treat patients with severe obesity and have fewer socioeconomic resources. In addition, although most private and public insurance companies cover the cost of the procedure and there are no differences in the effectiveness of therapy based on insurance status,46 patients with public insurance may face additional socioeconomic barriers to follow-up care, including the time and expense required to travel to and from those visits and resulting lost wages while attending appointments. Last, legacy effects related to the social stigma of surgery, safety concerns due to historically higher complication rates, and the multiple requirements to even qualify for bariatric surgery (eg, visits with psychologists, cardiologists, dieticians, and others to meet criteria) contribute to the implementation gap between science and practice.
Cost-Effectiveness of Obesity Therapies and Its Impact on Implementation
Studies demonstrate that despite significant public health efforts to address obesity, rates of obesity are not declining, and the poorer outcomes among individuals with obesity during the COVID-19 pandemic further highlight the need for successful methods for implementing obesity science into clinical practice.30 An important consideration that can stimulate or stall the implementation of scientific advancements in new treatments for obesity is cost-effectiveness. Among obesity treatments, bariatric surgery procedures consistently demonstrate cost savings, for example, reduced medical costs and expenditures.47 The cost-effectiveness of nonsurgical obesity treatment (behavioral and pharmacotherapy) has been demonstrated, although the findings are less consistent. This is due in part to lower degrees of weight loss and the challenges in quantifying the multifactorial and likely long-term or lagged benefits from these therapies.48,49 Studying the cost-effectiveness of obesity prevention is even more challenging.50 Still, this lack of definitive cost-effectiveness data likely contributes to the low uptake of obesity science implementation in clinical settings. The engagement of stakeholders, community partners, and health economists to help prospective design measurement of program costs and benefits in obesity science research is one strategy that could address this gap.51
The limited availability of cost-effectiveness and health outcomes data for obesity treatment relates to additional challenges in clinician reimbursement and patient costs for obesity treatment, which are significant obesity science implementation barriers. A recent qualitative study concluded that primary care clinicians believed that addressing obesity is an essential part of their job and that many find it feasible and rewarding. Yet, a lack of adequate reimbursement emerged as a primary barrier to these clinicians implementing obesity counseling in their practice.52 For example, policies in which patients must have a BMI ≥30 kg/m2 or clinical prediabetes before obesity services are reimbursable can impede and frustrate clinicians and patients who seek to prevent obesity or maintain obesity treatment successes. Furthermore, the limited availability of hard outcomes data (eg, cardiovascular outcomes, mortality) impedes convincing payers to reimburse treatments for obesity. On the other hand, outcomes trials cannot be reasonably conducted in lower-risk populations with obesity (i.e., younger people, those with no/minimal prevalent comorbidities) because of low event rates, high costs, and prolonged follow-up. Moreover, the lack of consensus on appropriate clinical parameters or quality benchmarks to define obesity-related outcomes (given its heterogeneity)24 that qualify for reimbursement further adds to clinician frustrations and thwarts the implementation of obesity management programs.23,53 For example, although cardiovascular outcomes and mortality are important, weight loss by itself may lead to more immediate improvements in quality of life and well-being that are not captured in outcomes used by payers to decide coverage. In addition, inadequate reimbursement for evidence-based behavioral treatments by nonphysicians (e.g., dieticians and psychologists) further limits the application of evidence-based behavioral treatments for obesity.20 Bariatric surgery is covered by Medicaid, but reimbursement has declined dramatically over the past decade, disincentivizing the provision of this effective treatment.54 Although questions about the cost-effectiveness and long-term outcomes of many obesity-related treatments remain, evidence for benefit is gradually emerging, and there is a gap between this body of evidence and the willingness of payers to cover treatments.50,53 This leads to a situation in which clinicians are not incentivized to provide obesity management services, resulting in the further widening of the implementation gap.
FOCUS ON RESOURCES TO FACILITATE IMPROVED POPULATION-LEVEL OBESITY MANAGEMENT
Despite advancements in understanding the causes and mechanisms that contribute to obesity, ongoing gaps in implementing evidence-based obesity science have impeded efforts to improve the quality, effectiveness, scalability, and equitability of successful obesity strategies into clinical practice. The following sections summarize existing and promising opportunities to address key implementation gaps and enable progress in the translation of obesity science into clinical practice for greater prevention, treatment, and control of this epidemic (Table).
![]()
Technology solutions to bridge the know-do gap in obesity prevention and treatment are promising, with emerging evidence to support multiple implementation strategies,55,56 including in many low- and middle-income countries that have seen the rapid adoption of digital technologies.57 Mobile health solutions, including popular weight loss applications (apps), are implementing various evidence-based behavior change techniques.58 However, the literature needs to be improved by better reporting of implementation strategies.59 Challenges with awareness, access, and engagement persist, especially in historically excluded groups who experience a high prevalence of obesity and disparities in care. One modeling study, for example, suggested that 75% awareness, 75% downloading, and 75% engagement with notifications may be required to achieve significant changes in physical activity and obesity prevalence among African American women in Washington, DC.60 Leveraging the increased access to telemedicine is another future opportunity to improve access to obesity specialists and treatments,56, especially in rural areas where the distance to the clinic is a major barrier.61 Increasing the use of inexpensive obesity-related health indicators such as routine measurement of the waist circumference as part of the standard vital signs or measurement of the supine sagittal abdominal diameter using sliding-beam calliper to estimate visceral adipose tissue burden62,63 clinically may shift the focus of obesity treatment from weight/BMI to risk-based markers. An even simpler tool for weight loss is regular (ie, weekly) self-weighing. Self-weighing as part of weight management programs has been shown to improve weight loss.64 Wireless scales allow remote monitoring of weight and transmission of weight data to clinicians, peers involved in group programs, and others to provide feedback, accountability, and support.65
Barriers to Commercial and Community Resources Must Be Addressed
In addition to a multilevel need to improve referrals and equitable access to clinical weight management programs and other treatment options, future implementation work needs to emphasize connections to programs outside clinical settings. Some commercial weight loss programs can be effective, but access is often limited by cost, distance, and patient perceptions of safety and belonging. Nonprofit community programs like the YMCA or Take Off Pounds Sensibly66 may be more acceptable and affordable than medical or commercial options. These programs offer tangible and structured support for weight loss or maintenance and often serve as a link to social support as well. Strategies to inform patients and clinicians about which programs are available in their area and which might be appropriate according to different patient factors may enhance equitable reach and quality of health services delivery but need to be developed and tested at scale.
Targeting the Patient’s Broader Social Support Network to Promote Broader, More Comprehensive Implementation of Obesity-Focused Strategies
Although much of the evidence available for successful weight loss and maintenance programs comes from individual-level clinical trials, there is increasing acknowledgement that lifestyle changes may be more likely to succeed if implemented at the couple, family, or household level. 67–69 The importance of social support for success is well recognized, even for pharmacological and surgical treatments that are inherently implemented at the individual level. Behaviors and environments that contribute to obesity are often shared among those with close social connections, and unsurprisingly, attempts to modify behavior without influencing other sociological factors that contribute to obesity in the first place are often unsuccessful. Despite this growing understanding, widespread implementation of successful programs is rare, and accessibility and acceptability in underrepresented racial and ethnic populations that commonly impede the implementation of weight-modifying programs are often overlooked.70 Although clinicians care for individual patients with obesity, patients are part of families and communities. A patient’s social environment has a great deal of influence on their weight, and clinicians need to recognize and assess this broader context, as well as for programs to consider sociological factors. Here is an example: A community-based program must take into consideration what food sources are available at a reasonable cost to participants in the vicinity to be practical and effective.
More Evaluation Is Needed to Support Health Policy Change, Implementation, and Scalability
Health policy changes are essential to increase the provision of available evidence-based strategies such as behavioral therapy, pharmacotherapy, and bariatric surgery to the large population of individuals with or at risk for obesity who critically need these services.30 Efforts to provide evidence-based coverage for the treatment of obesity are often inhibited by current legislation in the US Congress. Despite recent important advancements in obesity pharmacotherapy coverage by Medicare Part D for individuals with existing CVD to reduce adverse cardiovascular events, further action is needed. Efforts led by the Treat and Reduce Obesity Act to expand Medicare coverage, including screening and treatment of obesity for a broader range of healthcare clinicians, as well as providing coverage for FDA-approved medications for long-term weight management, have stalled at the federal level over the past decade.71 This underscores the persistent challenges in achieving universal coverage for AOMs, despite notable progress in addressing specific patient populations, such as those with existing CVD who are at the highest risk for adverse cardiovascular outcomes. Several professional societies and stakeholders are currently engaged in efforts to lobby for health policy changes to make obesity treatment more accessible and affordable for patients with obesity at high risk for developing CVD.
Further evaluation is needed to support policy implementation and scalability. Evidence on implementation costs and cost-effectiveness will be integral to policy implementation efforts and systemic change. Because they can be more rapidly scaled with fewer human resources, digital interventions may prove particularly cost-effective, as shown in a recent analysis of adolescent obesity interventions.72 This is particularly true for resource-constrained health systems worldwide, where health departments will continue to focus on “best buys” to address an epidemic of noncommunicable diseases.73,74 Lastly, forming a shared resource library accessible to all clinicians engaged in obesity care might help clinicians connect patients to resources and offer connections that might be the best fit for each patient. Establishing such resources and evaluating their effectiveness is only one example of a future goal for implementing obesity science into clinical practice. Given the widespread increase in obesity prevalence worldwide, attention to global implementation strategies, each with its unique geographic challenges, will be important to address the implementation gap of obesity science in practice worldwide in the future.
CONCLUSIONS
The science of obesity is a relatively young field, gaining traction in the 1970s when the prevalence of obesity among men and women of all ethnic groups, ages, and educational and socioeconomic levels started to increase.75 Despite decades of advancement in our scientific understanding of the pathophysiology underlying obesity and its potential treatment, a substantial gap between that knowledge and the successful implementation of obesity science to treat obesity within clinical practice remains. It is equally important to recognize that the lack of sufficient implementation of evidence-informed science into practice, albeit largely evidenced in adults, is magnified in the pediatric and adolescent populations, wherein identifying and managing overweight or obesity is vital to preventing the development of long-term obesity and its sequelae.76 Determining when and how to implement obesity-targeted therapies for maximum effectiveness remains challenging. Identification of barriers to implementing guideline-driven care and prompt discussions about solutions are needed to ensure that patients in greatest need have access to appropriate therapies. To reach and successfully affect these populations in need, clinicians may consider how the social determinants of health, including insurance type, health literacy, access to health-promoting resources, and social support influence the likelihood of successful treatment. Addressing the barriers to the successful implementation of obesity science into practice requires investment in methodologies proven to narrow the know-do gap that includes education about the complex origins and clinical consequences of obesity, a framework for the delivery of obesity care, and health policy interventions that are essential to the success of applying obesity science to the individual patient. Healthcare systems can contribute to the success of implementation by coordinating care teams into fewer visits to reduce the burden on patients who would find themselves coming for multiple visits and scheduling with numerous specialists. Comprehensive care teams that include various health care professionals, in addition to social workers and social services personnel, are essential to addressing nonmedical barriers to successful implementation. Public policy should align with implementation efforts to further support the research and evaluation needed to drive policy implementation and scalability. Evidence for implementation costs and cost-effectiveness will be integral to prioritizing policy implementation efforts and systemic change. Funding to promote and sustain such research is vital to the success and reach of these endeavors. Last, there is an urgent need for better education and training in implementing science in obesity medicine. Building obesity care around these principles requires substantial financial input and engagement from multiple stakeholders. Still, the rewards of lower mortality, long-term healthcare cost savings, and improved quality of life warrant the investment.
References
1. Fryar CD, Carroll MD, Afful J. Prevalence of overweight, obesity, and severe obesity among adults aged 20 and over: United States, 1960–1962 through 2017–2018. NCHS Health E-Stats. 2020:1–7.
2. Li HL, Tsoi MF, Feng Q, Cheung C-L, Cheung T, Cheung BM. Prevalence of childhood obesity in the United States 1999-2018: a 20-year analysis. J Endocr Soc. 2021;5:A24. Abstract.
3. Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, Boehme AK, Buxton AE, Carson AP, Commodore-Mensah Y, et al. Heart disease and stroke statistics—2022 update: a report from the American Heart Association [published correction appears in Circulation. 2022;146:e141]. Circulation. 2022;145:e153–e639. doi: 10.1161/CIR.0000000000001052
4. Ward ZJ, Bleich SN, Cradock AL, Barrett JL, Giles CM, Flax C, Long MW, Gortmaker SL. Projected US state-level prevalence of adult obesity and severe obesity. N Engl J Med. 2019;381: 2440– 2450. doi: 10.1056/NEJMsa 1909301
5. Mohebi R, Chen C, Ibrahim NE, McCarthy CP, Gaggin HK, Singer DE, Hyle EP, Wasfy JH, Januzzi JL. Cardiovascular disease projections in the United States based on the 2020 census estimates. J Am Coll Cardiol. 2022;80:565–578. doi: 10.1016/j.jacc. 2022.05.033
6. Carnethon MR, Pu J, Howard G, Albert MA, Anderson CAM, Bertoni AG, Mujahid MS, Palaniappan L, Taylor HA, Willis M, et al; on behalf of the American Heart Association Council on Epidemiology and Prevention; Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; Council on Functional Genomics and Translational Biology; and Stroke Council. Cardiovascular health in African Americans: a scientific statement from the American Heart Association.Circulation.2017;136: e393–e423. doi: 10.1161/CIR.000000 0000000534
7. Johnston CA, Moreno JP. Bridging the science-practice gap in obesity treatment. Am J Lifestyle Med. 2016;10:100–103. doi: 10.1177/ 1559827615620381
8. Kaiser KA, Carson TL, Dhurandhar EJ, Neumeier WH, Cardel MI. Biobehavioural approaches to prevention and treatment: A call for implementation science in obesity research. Obes Sci Pract. 2020;6:3–9. doi: 10.1002/osp4.384
9. Tabak RG, Khoong EC, Chambers DA, Brownson RC. Bridging research and practice: models for dissemination and implementation research. Am J Prev Med. 2012;43:337–350. doi: 10.1016/j.amepre.2012.05.024
10. Alcaraz KI, Yanez BR. Interventions to promote health equity: implications for implementation science in behavioral medicine. Transl Behav Med. 2022; 12:885–888. doi: 10.1093/tbm/ ibac062
11. Holtrop JS, Rabin BA, Glasgow RE. Dissemination and implementation science in primary care research and practice: contributions and opportunities. J Am Board Family Med. 2018;31:466–478. doi: 10.3122/jabfm.2018.03.170259
12. Kwan BM, McGinnes HL, Ory MG, Estabrooks PA, Waxmonsky JA, Glasgow RE. RE-AIM in the real world: use of the RE-AIM framework for program planning and evaluation in clinical and community settings. Front Public Health. 2019;7:345. doi: 10.3389/fpubh.2019.00345
13. Yarlagadda S, Townsend MJ, Palad CJ, Stanford FC. Coverage of obesity and obesity disparities on American Board of Medical Specialties (ABMS) examinations. J Natl Med Assoc. 2021;113:486–492. doi: 10.1016/j. jnma.2021.03.004
14. Mastrocola MR, Roque SS, Benning LV, Stanford FC. Obesity education in medical schools, residencies, and fellowships throughout the world: a systematic review. Int J Obes (Lond). 2020;44:269–279. doi: 10.1038/s41 366-019-0453-6
15. Gudzune KA, Wickham EP, Schmidt SL, Stanford FC. Physicians certified by the American Board of Obesity Medicine provide evidence-based care. Clin Obes. 2021;11:e12407. doi: 10.1111/cob. 12407
16. Fitzpatrick SL, Wischenka D, Appelhans BM, Pbert L, Wang M, Wilson DK, Pagoto SL, Medicine SB. An Evidence-based guide for obesity treatment in primary care. Am J Med. 2016;129: 115.e1–115.e7.
17. Laddu D, Ma J, Kaar J, Ozemek C, Durant RW, Campbell T, Welsh J, Turrise S; on behalf of the American Heart Association Behavioral Change for Improving Health Factors Committee of the Council on Epidemiology and Prevention and the Council on Lifestyle and Cardiometabolic Health; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Hypertension; and Stroke Council. Health behavior change programs in primary care and community practices for cardiovascular disease prevention and risk factor management among midlife and older adults: a scientific statement from the American Heart Association. Circulation. 2021;144: e533–e549. doi: 10.1161/CIR.0000 000000001026
18. Kris-Etherton PM, Petersen KS, Després JP, Anderson CAM, Deedwania P, Furie KL, Lear S, Lichtenstein AH, Lobelo F, Morris PB, et al; on behalf of the American Heart Association Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular and Stroke Nursing; Stroke Council; Council on Clinical Cardiology; Council on Arteriosclerosis, Thrombosis and Vascular Biology; and Council on Hypertension. Strategies for promotion of a healthy lifestyle in clinical settings: pillars of ideal cardiovascular health: a science advisory from the American Heart Association. Circulation. 2021; 144:e495–e514. doi: 10.1161/CIR.00 00000000001018
19. O’Connor EA, Evans CV, Rushkin MC, Redmond N, Lin JS. Behavioral counseling to promote a healthy diet and physical activity for cardiovascular disease prevention in adults with cardiovascular risk factors: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA.2020;324:2076 –2094. doi: 10.1001/jama.2020.17108
20. Ockene JK, Ashe K, Peterson KS, Fitzgibbon M, Buscemi J, Dulin A. Society of Behavioral Medicine call to action: include obesity/overweight management education in health professional curricula and provide coverage for behavior-based treatments of obesity/overweight most commonly provided by psychologists, dieticians, counselors, and other health care professionals and include such providers on all multidisciplinary teams treating patients who have overweight or obesity. Transl Behav Med. 2021;11: 653–655. doi: 10.1093/tbm/ibaa030
21. National Academies of Sciences, Engineering, and Medicine. Roundtable on Obesity Solutions: Year in Review 2022. Accessed August 3, 2023. https://nap.nationalacademies.org/catalog/26855/roundtable-on-obesity-solutions-year-in-review-2022
22. Lloyd-Jones DM, Allen NB, Anderson CA, Black T, Brewer LC, Foraker RE, Grandner MA, Lavretsky H, Perak AM, Sharma G, et al; on behalf of the. American Heart Association. Life’s Essential 8: updating and enhancing the American Heart Association’s construct of cardiovascular health: a presidential advisory from the American Heart Association. Circulation. 2022;146:e18–e43. doi: 10.1161/CIR.0000000000001078
23. Stefan N, Häring H-U, Schulze MB. Metabolically healthy obesity: the low-hanging fruit in obesity treatment? Lancet Diabetes Endocrinol.2018; 6:249–258. doi: 10.1016/S2213-8587(17)30292-9
24. Piché M-E, Tchernof A, Després J-P. Obesity phenotypes, diabetes, and cardiovascular diseases. Circ Res. 2020; 126:1477–1500. doi: 10.1161/ CIRCRESAHA.120.316101
25. Powell-Wiley TM, Poirier P, Burke LE, Després J-P, Gordon-Larsen P, Lavie CJ, Lear SA, Ndumele CE, Neeland IJ, Sanders P, et al; on behalf of the American Heart Association Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; Council on Epidemiology and Prevention; and Stroke Council. Obesity and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2021;143:e984–e1010. doi: 10.1161/ CIR.0000000000000973
26. Turner M, Jannah N, Kahan S, Gallagher C, Dietz W. Current knowledge of obesity treatment guidelines by health care professionals. Obesity (Silver Spring). 2018;26:665–671. doi: 10.1002/oby.22142
27. Lewis KH, Gudzune KA, Fischer H, Yamamoto A, Young DR. Racial and ethnic minority patients report different weight-related care experiences than non-Hispanic Whites. Prev Med Rep. 2016;4:296–302. doi: 10.1016/j. pmedr.2016.06.015
28. Chen J, Mullins CD, Novak P, Thomas SB. Personalized strategies to activate and empower patients in health care and reduce health disparities. Health Educ Behav. 2016;43:25–34. doi: 10.1177/1090198115579415
29. Dhanani S, Ramlakhan JU, Berta WB, Gagliardi AR. Optimizing the design and implementation of question prompt lists to support person-centred care: a scoping review. Health Expect. 2023;26:1404–1417. doi: 10.1111/hex. 13783
30. Kyle TK, Stanford FC. Moving toward health policy that respects both science and people living with obesity. Nurs Clin North Am. 2021;56:635–645. doi: 10.1016/j.cnur.2021.08.003
31. Ghusn W, De la Rosa A, Sacoto D, Cifuentes L, Campos A, Feris F, Hurtado MD, Acosta A. Weight loss outcomes associated with semaglutide treatment for patients with overweight or obesity. JAMA Netw Open. 2022;5:e2231982. doi: 10.1001/jamanetworkopen.2022. 31982
31a. Jastreboff AM, Aronne LJ, Ahmad NN, Wharton S, Connery L, Alves B, Kiyosue A, Zhang S, Liu B, Bunck MC, et al; SURMOUNT-1 Investigators. Tirzepatide once weekly for the treatment of obesity. N Engl J Med. 2022;387:205–216. doi: 10.1056/NEJMoa2206038
32. Claridy MD, Czepiel KS, Bajaj SS, Stanford FC. Treatment of obesity: pharmacotherapy trends of office-based visits in the United States From 2011 to 2016. Mayo Clin Proc. 2021;96: 2991–3000. doi: 10.1016/j.mayocp. 2021.07.021
33. US Government Accountability Office. Obesity drugs: few adults used prescription drugs for weight loss and insurance coverage varied GAO-19-577. Accessed December 23, 2022. https://gao.gov/products/GAO-19-577
34. Curry SJ, Krist AH, Owens DK, Barry MJ, Caughey AB, Davidson KW, Doubeni CA, Epling JW, Grossman DC, Kemper AR, et al; US Preventive Services Task Force. Behavioral weight loss interventions to prevent obesity-related morbidity and mortality in adults: US Preventive Services Task Force recommendation statement. JAMA. 2018;320:1163–1171. doi: 10.1001/jama.2018.13022
35. Gomez G, Stanford FC. US health policy and prescription drug coverage of FDA-approved medications for the treatment of obesity. Int J Obes (Lond). 2018;42:495–500. doi: 10.1038/ijo.2017.287
35a.Lincoff AM, Brown-Frandsen K, Colhoun HM, Deanfield J, Emerson SS, Esbjerg S, Hardt-Lindberg S, Hovingh GK, Kahn SE, Kushner RF, et al; SELECT Trial Investigators. Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023; 389:2221–2232. doi: 10.1056/NEJMoa 2307563
36. Phillips BT, Shikora SA. The history of metabolic and bariatric surgery: development of standards for patient safety and efficacy. Metab Clin Exp. 2018;79:97–107. doi: 10.1016/j. metabol.2017.12.010
37. Liao J, Yin Y, Zhong J, Chen Y, Chen Y, Wen Y, Cai Z. Bariatric surgery and health outcomes: an umbrella analysis. Front Endocrinol (Lausanne). 2022; 13:1016613. doi: 10.3389/fendo. 2022.1016613
38. Sheng B, Truong K, Spitler H, Zhang L, Tong X, Chen L. The long-term effects of bariatric surgery on type 2 diabetes remission, microvascular and macrovascular complications, and mortality: a systematic review and meta-analysis. ObesSurg.2017;27: 2724–2732. doi: 10.1007/s11695-017-2866-4
39. Aggarwal R, Harling L, Efthimiou E, Darzi A, Athanasiou T, Ashrafian H. The effects of bariatric surgery on cardiac structure and function: a systematic review of cardiac imaging outcomes. Obes Surg. 2016;26: 1030–1040. doi: 10.1007/s11695-015-1866-5
40. Arterburn DE, Telem DA, Kushner RF, Courcoulas AP. Benefits and risks of bariatric surgery in adults: a review. JAMA. 2020;324:879–887. doi: 10.1001/jama.2020.12567
41. Chalklin CG, Ryan Harper EG, Beamish AJ. Metabolic and bariatric surgery in adolescents. Curr Obes Rep. 2021; 10:61–69. doi: 10.1007/s13679-021-00423-3
42. Hecht LM, Pester B, Braciszewski JM, Graham AE, Mayer K, Martens K, Hamann A, Carlin AM, Miller-Matero LR. Socioeconomic and racial disparities in bariatric surgery. Obes Surg. 2020; 30:2445–2449. doi: 10.1007/s11695-020-04394-7
43. Bhogal SK, Reddigan JI, Rotstein OD, Cohen A, Glockler D, Tricco AC, Smylie JK, Glazer SA, Pennington J, Conn LG, et al. Inequity to the utilization of bariatric surgery: a systematic review and meta-analysis. Obes Surg. 2015; 25:888–899. doi: 10.1007/s11 695-015-1595-9
44. Miller-Matero LR, Hecht L, Patel S, Martens KM, Hamann A, Carlin AM. The influence of health literacy and health numeracy on weight loss outcomes following bariatric surgery. Surg Obes Relat Dis. 2021;17:384 – 389. doi: 10.1016/j.soard.2020. 09.021
45. Morche J, Mathes T, Pieper D. Relationship between surgeon volume and outcomes: a systematic review of systematic reviews. Syst Rev. 2016;5: 204. doi: 10.1186/s13643-016-0376-4
46. Liu N, Venkatesh M, Hanlon BM, Muraveva A, Johnson MK, Hanrahan LP, Funk LM. Association between Medicaid status, social determinants of health, and bariatric surgery outcomes. Ann Surg Open. 2021;2:e028. doi: 10.1097/AS9.0000000000000028
47. Xia Q, Campbell JA, Ahmad H, Si L, de Graaff B, Palmer AJ. Bariatric surgery is a cost-saving treatment for obesity: a comprehensive meta-analysis and updated systematic review of health economic evaluations of bariatric surgery. Obes Rev. 2020;21:e12932. doi: 10.1111/obr.12932
48. Jacobsen E, Boyers D, Avenell A. Challenges of systematic reviews of economic evaluations: a review of recent reviews and an obesity case study. Pharmacoeconomics. 2020;38:259–267. doi: 10.1007/ s40273-019-00878-2
49. Jacobsen E, Boyers D, Manson P, Avenell A. A systematic review of the evidence for non-surgical weight management for adults with severe obesity: what is cost-effective and what are the implications for the design of health services? Curr Obes Rep. 2022;11:356–385. doi: 10.1007 /s13679-022-00483-z
50. Ananthapavan J, Sacks G, Moodie M, Carter R. Economics of obesity: learning from the past to contribute to a better future. Int J Environ Res Public Health. 2014;11:4007–4025. doi: 10.3390/ijerph110404007
51. Daumit GL, Janssen EM, Jerome GJ, Dalcin AT, Charleston J, Clark JM, Coughlin JW, Yeh HC, Miller ER, Durkin N, et al. Cost of behavioral weight loss programs implemented in clinical practice: the POWER trial at Johns Hopkins. Transl Behav Med. 2020;10:103–113. doi: 10.1093/tbm/ iby120
52. Nederveld A, Phimphasone-Brady P, Connelly L, Fitzpatrick L, Holtrop JS. The joys and challenges of delivering obesity care: a qualitative study of US primary care practices. J Gen Intern Med. 2021;36:2709–2716. doi: 10.1007/s11606-020-06548-w
53. Baum C, Andino K, Wittbrodt E, Stewart S, Szymanski K, Turpin R. The challenges and opportunities associated with reimbursement for obesity pharmacotherapy in the USA. Pharmacoeconomics. 2015;33:643– 653. doi: 10.1007/s40273-015-0264-0
54. Zhong A, Bajaj SS, Khunte M, Dang N, Stanford FC. Trends in metabolic and bariatric surgery reimbursement in the USA. Obes Surg. 2022;32: 4110– 4112. doi: 10.1007/s11695-022-06329-w
55. Dounavi K, Tsoumani O. Mobile health applications in weight management: a systematic literature review. Am J Prev Med. 2019;56:894–903. doi: 10.1016/j.amepre.2018.12.005
56. Kahan S, Look M, Fitch A. The benefit of telemedicine in obesity care. Obesity (Silver Spring). 2022;30:577–586. doi: 10.1002/oby.23382
57. Reddy P, Dukhi N, Sewpaul R, Ellahebokus MAA, Kambaran NS, Jobe W. Mobile health interventions addressing childhood and adolescent obesity in sub-Saharan Africa and Europe: current landscape and potential for future research. Front Public Health. 2021;9:604439. doi: 10.3389/fpubh.2021.604439
58. Vlahu-Gjorgievska E, Burazor A, Win KT, Trajkovik V. mHealth apps targeting obesity and overweight in young people: app review and analysis. JMIR Mhealth Uhealth. 2023;11:e37716. doi: 10.2196/37716
59. Encantado J, Palmeira AL, Silva C, Sniehotta FF, Stubbs RJ, Gouveia MJ, Teixeira PJ, Heitmann BL, Marques MM. What goes on in digital behaviour change interventions for weight loss maintenance targeting physical activity: a scoping review. Digit Health. 2022;8:20552076221129089. doi: 10.1177/20552076221129089
60. Powell-Wiley TM, Martinez MF, Tamura K, Neally SJ, O’Shea KJ, Curlin K, Albarracin Y, Vijayakumar NP, Morgan M, Ortiz-Chaparro E, et al. The impact of a place-tailored digital health app promoting exercise classes on African American women’s physical activity and obesity: simulation study. J Med Internet Res. 2022;24:e30581. doi: 10.2196/30581
61. Gray KE, Rao M, Gunnink E, Eschenroeder L, Geyer JR, Nelson KM, Reddy A. Home telehealth in the Veterans Health Administration: trends and correlates of length of enrollment from 2010 to 2017. J Gen Intern Med. 2022;37: 3089–3096. doi: 10.1007/s11606-022-07452-1
62. Kullberg J, von Below C, Lönn L, Lind L, Ahlström H, Johansson L. Practical approach for estimation of subcutaneous and visceral adipose tissue. Clin Physiol Funct Imaging. 2007;27:148– 153. doi: 10.1111/j.1475-097X.2007. 00728.x
63. Yim JY, Kim D, Lim SH, Park MJ, Choi SH, Lee CH, Kim SS, Cho SH. Sagittal abdominal diameter is a strong anthropometric measure of visceral adipose tissue in the Asian general population. Diabetes Care. 2010; 33:2665–2670. doi: 10.2337/dc10-0606
64. Zheng Y, Klem ML, Sereika SM, Danford CA, Ewing LJ, Burke LE. Self-weighing in weight management: a systematic literature review. Obesity (Silver Spring). 2015;23:256–265. doi: 10.1002/oby.20946
65. Miller NA, Ehmann MM, Hagerman CJ, Forman EM, Arigo D, Spring B, LaFata EM, Zhang F, Milliron B-J, Butryn ML. Sharing digital self-monitoring data with others to enhance long-term weight loss: a randomized controlled trial. Contemp Clin Trials. 2023; 129:107201. doi: 10.1016/j.cct.2023. 107201
66. Mitchell NS, Dickinson LM, Kempe A, Tsai AG. Determining the effectiveness of Take Off Pounds Sensibly (TOPS), a nationally available nonprofit weight loss program. Obesity (Silver Spring). 2011;19:568–573. doi: 10.1038/oby. 2010.202
67. Cobb LK, Godino JG, Selvin E, Kucharska-Newton A, Coresh J, Koton S. Spousal influence on physical activity in middle-aged and older adults: the ARIC study. Am J Epidemiol. 2016; 183:444–451. doi: 10.1093 je/kwv1 04
68. Cobb LK, McAdams-DeMarco MA, Gudzune KA, Anderson CA, Demerath E, Woodward M, Selvin E, Coresh J. Changes in body mass index and obesity risk in married couples over 25 years: the ARIC cohort study. Am J Epidemiol. 2016;183:435–443. doi: 10.1093/aje/kwv112
69. Skapinsky KF, Persky S, Lewis M, Goergen A, Ashida S, de Heer HD, Hadley D, Wilkinson AV, Koehly LM. Heart disease risk information, encouragement, and physical activity among Mexican-origin couples: self- or spouse-driven change? Transl Behav Med. 2018;8:95–104. doi: 10.1093/tbm/ibx012
70. Wang X, Ammerman A, Orr CJ. Family-based interventions for preventing overweight or obesity among preschoolers from racial/ethnic minority groups: a scoping review. Obes Sci Pract. 2022;8:371–386. doi: 10.1002/osp4.578
71. Bajaj SS, Jain B, Kyle TK, Gallagher C, Stanford FC, Srivastava G. Overcoming congressional inertia on obesity requires better literacy in obesity science. Obesity (Silver Spring). 2022;30:799–801. doi: 10.1002/oby. 23405
72. Carrello J, Hayes A, Baur LA, Lung T. Potential cost-effectiveness of e-health interventions for treating overweight and obesity in Australian adolescents. Pediatr Obes. 2023;18 :e13003. doi: 10.1111/ijpo.13003
73. Bertram MY, Chisholm D, Watts R, Waqanivalu T, Prasad V, Varghese C. Cost-effectiveness of population level and individual level interventions to combat non-communicable disease in eastern sub-Saharan Africa and South East Asia: a WHO-CHOICE analysis. Int J Health Policy Manag. 2021;10:724–733. doi: 10.34172/ ijhpm. 2021.37
74. Uwimana-Nicol J, Hendricks L, Young T. Population-level interventions targeting risk factors of diabetes and hypertension in South Africa: a document review. BMC Public Health. 2021;21:2283. doi: 10.1186/ s12889-021-11910-6
75. Zhang Q, Wang Y. Trends in the association between obesity and socioeconomic status in U.S. adults: 1971 to 2000. Obes Res. 2004;12:16 22–1632. doi: 10.1038/oby.2004.202
76. O’Connor EA, Evans CV, Burda BU, Walsh ES, Eder M, Lozano P. Screening for obesity and intervention for weight management in children and adolescents: evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2017;317: 2427–2444. doi: 10.1001/jama.2017. 0332