

Magnus Michael Sichalwea b, Abdul Basit d, Attiq Ur Rehman d, Grace Tavengana b, Manas Ranjan Behera c, Muskan Fatima b, Phephile Patience Sifundza b
a Division of Health, Nutrition and Social Welfare Services, Butiama District Council, Mara, Tanzania
b School of Public Health, Nantong University, Jiangsu, China
c School of Public Health, Kalinga Institute of Industrial Technology (KIIT) Deemed to be University, Bhubaneswar, 751024, India
d School of Nursing and Rehabilitation, Nantong University, Jiangsu, China
Highlights
• Cervical cancer screening uptake in SSA remains critically low at below 15 %
• Health system gaps, stigma, and inequities drive low screening coverage.
• Task-shifting and provider training improve screening access and quality.
• Mobile clinics and service integration expand reach in under served areas.
• System-level investment is key to equitable cervical cancer elimination.
Abstract
Cervical cancer remains a major public health problem, causing over 340,000 deaths in 2020, with nearly 90 % occurring in low- and middle-income countries. Sub-Saharan Africa (SSA) carries the highest burden due to weak health systems, limited HPV vaccination, and very low screening coverage. This review, conducted following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, synthesized evidence from thirty recent studies and found that screening uptake in SSA remains extremely low (10–19 %, pooled 12.9 %), constrained by limited access to facilities, personnel shortages, inadequate equipment, socioeconomic inequities, weak supply chains, low provider guideline awareness, cultural stigma, and high loss to follow-up. Promising strategies to address these barriers include task-shifting to nurses and community health workers, structured training and supervision, mobile clinics, community outreach, and emerging technologies such as AI-powered diagnostics. With targeted investment, political commitment, and adaptation of proven global strategies, SSA can strengthen screening, improve equity, and move closer to eliminating cervical cancer as a public health threat.
Keywords
Cervical cancer; Screening; Healthcare infrastructure; Sub-Saharan Africa; Low-resource settings
Background
Cervical cancer is the fourth most common malignancy in women worldwide, with 604,127 new cases and 342,000 deaths reported in 2020, the majority occurring in low and middle-income countries (LMICs) (Singh et al., 2023, Sung et al., 2021). The highest incidence rates are in Eastern, Southern, and Middle Africa, where cervical cancer remains the leading cause of cancer-related death among women (Sung et al., 2021). Early detection through timely screening and treatment can prevent most cases and deaths, yet screening coverage in LMICs averages only 19 %, compared to 63 % in high income countries (HICs) (Petersen et al., 2022). Barriers include limited awareness, socio-cultural factors, and systemic healthcare challenges (Petersen et al., 2022, Singh et al., 2023).
Persistent infection with carcinogenic Human Papillomavirus (HPV) strains, particularly types 16 and 18, accounts for 70–75 % of cervical cancers and 40–60 % of precancerous lesions (NCI, 2022). HPV vaccination and screening, combined with treatment strategies such as Visual Inspection with Acetic Acid (VIA) followed by cryotherapy or thermo-coagulation, are highly effective preventive approaches in low-resource settings (Campos et al., 2024). High income countries have substantially reduced cervical cancer burden through widespread vaccination, organised screening programs, and advanced treatments (ROCHE, 2025).
In Sub-Saharan Africa (SSA), the disease burden is exacerbated by limited HPV vaccination, low screening uptake, HIV co-infection, and socio-cultural barriers (Bruni et al., 2022, WHO, 2024). Strengthening health- care infrastructure is key to improving access to vaccination, screening, and treatment, and to achieving the World Health Organization (WHO) 2030 cervical cancer elimination targets of 90 % vaccination, 70 % screening, and 90 % treatment coverage (WHO, 2024). The WHO health system framework identifies six pillars essential for effective care: service delivery, workforce, information systems, medical products and technologies, financing, and leadership (Health system building blocks, 2023). Weaknesses in these areas, such as staff shortages and limited screening technologies, contribute to high cervical cancer incidence in SSA (Healthcare Infra- structure, 2023; Singh et al., 2023). Successful models like Rwanda’s HPV vaccination program and Zambia’s integration of screening into HIV care show how strong infrastructure, trained personnel, and functional tools (VIA, Pap smears, HPV testing) enhance outcomes (Binagwaho et al., 2012, Sahasrabuddhe et al., 2012). Robust healthcare infrastructure remains vital for effective screening in low-resource settings (Healthcare Infrastructure, 2023). This review examines the role of healthcare infrastructure in enabling cervical cancer screening in SSA.
Methodology
Search strategy
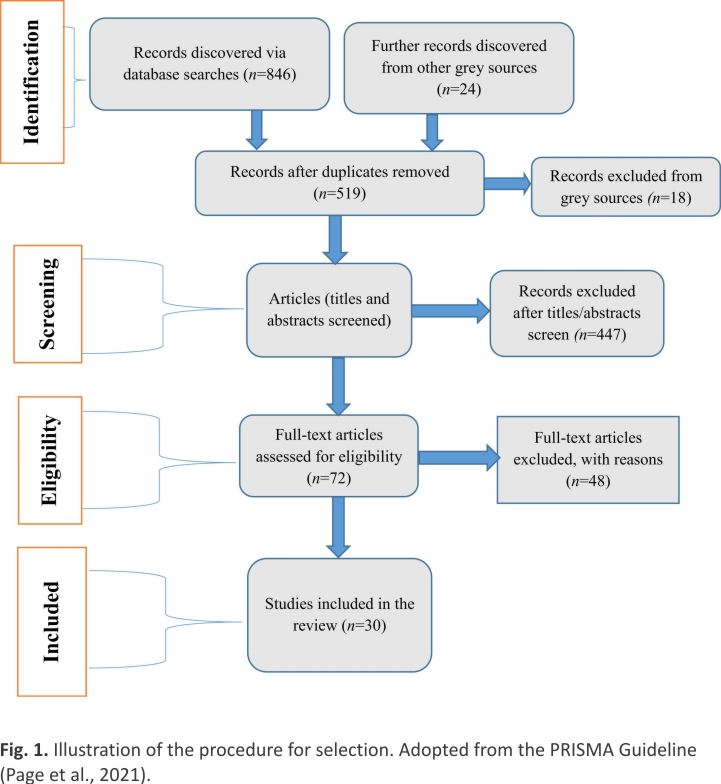
A systematic literature search was conducted in May 2025 following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021) across six databases: Ovid MEDLINE, Embase, PubMed, PsycINFO, Google Scholar, and Scopus. The search focused on Cervical Cancer Screening (CCS) in SSA, examining system-level facilitators and barriers such as healthcare infrastructure, workforce capacity, and screening equipment functionality. The strategy centred on three themes: (1) accessibility and geographic distribution of CCS services, (2) provider capacity, training, and competencies, and (3) availability and maintenance of screening devices. Both MeSH and free-text terms were combined with Boolean operators (“AND”/“OR”), including keywords like “visual inspection with acetic acid (VIA),” “Pap smear,” “HPV test,” “cervical cancer screening,” “health infrastructure,” and regional terms such as “West Africa,” “East Africa,” and “Sub-Saharan Africa.” Example search strings included “cervical cancer screening” AND (“healthcare infrastructure” OR “geographic access”) and “screening equipment” AND “Sub-Saharan Africa.” Only English-language studies from low-resource SSA settings were included.
Facility mapping studies and national surveys informed service distribution; qualitative and quantitative studies explored referral systems, transport, and outreach models; workforce assessments examined provider training and distribution; and implementation studies assessed the availability and performance of screening technologies. Search results were managed in Zotero for deduplication, with titles and abstracts screened for relevance before full-text review. Additional grey literature was identified through ProQuest Theses, reference lists, and expert consultation.
Eligibility criteria
Studies examining system-level healthcare infrastructure affecting CCS in low-income SSA countries were eligible. Included studies addressed facility readiness, functional screening technologies (Pap smear, VIA, HPV tests), and trained healthcare providers, and used systematic review, cohort, cross-sectional, qualitative, or mixed-method designs. Only English-language studies from the past decade conducted in SSA were considered. Key factors included equipment availability, staffing, training, and health system organization. Studies focusing solely on individual-level factors were excluded.
Exclusion criteria
Studies published before the last decade, not in English, lacking full-text availability, or not addressing healthcare infrastructure in SSA CCS programs were excluded.
Data selection and synthesis
The initial search yielded 846 articles. After deduplication, 327 duplicate records were removed, leaving 519 articles for screening. Following title and abstract review, 72 full texts were assessed, with 24 peer-reviewed studies published between 2005 and 2024 meeting eligibility criteria. Six grey literature sources (published between 2015 and 2024) were added, resulting in 30 studies for synthesis. Table 1 summarises study details, CCS methods, and infrastructure and workforce challenges, barriers, and facilitators. Included studies comprised qualitative research on women’s and providers’ experiences, quantitative studies on coverage and program outcomes, and reviews or meta-analyses. Grey literature sources included WHO Regional Office for Africa reports (2022, 2024), the Atlas of African Health Statistics, African Development Bank (2022)–(2030), World Bank (2023), and Pew Research Centre. Narrative synthesis was used to identify key infrastructural influences on CCS performance in resource-limited SSA settings.

This study is a systematic review of published literature and did not involve primary data collection from human participants or animals. Therefore, formal ethical approval was not required. All included studies were cited appropriately, and their findings are presented in accordance with ethical research and reporting standards.
The accessibility of healthcare facilities and their impact on CCS Programs
Accessibility to healthcare facilities plays a significant role as a determinant of the coverage and effectiveness of cervical cancer screening programs in SSA’s under-resourced regions. Some interdependent factors illustrate this impact:
Limited access to and healthcare infrastructure
Access to healthcare facilities strongly influences CCS coverage and effectiveness in SSA. It encompasses geographic distance, service costs, provider availability, awareness, and cultural or systemic barriers. Screening rates in SSA remain low, averaging 10–11 %, mainly due to limited access to adequately equipped facilities (Dzinamarira et al., 2023, Yang et al., 2023). Most countries lack national screening programs and rely on low-cost methods such as VIA, while more sensitive tests like Pap smears and HPV DNA testing remain unaffordable (Ba et al., 2021, Burt et al., 2021, Dzinamarira et al., 2023, Petersen et al., 2022, Simms et al., 2023). Overall coverage ranges from 10 % to 19 %, with wide disparities (0.7 % in Benin to 45.9 % in Namibia) (Asgedom et al., 2024, Ba et al., 2021, Yimer et al., 2021).
Educational, economic, and geographic inequalities further restrict access (Asgedom et al., 2024, Sichalwe, 2025). Rural, low-income, and less-educated women face barriers such as limited facilities, poor transport, and low awareness (Burt et al., 2021, Sichalwe, 2025). Economic hardship and out-of-pocket costs exacerbate exclusion and delay diagnosis (Asgedom et al., 2024, Sichalwe, 2025).
Competing health priorities and resource constraints
The WHO African Region faces a “triple burden” of communicable diseases, noncommunicable diseases, and injuries, with infectious and maternal conditions consuming most health resources (Atlas of African Health Statistics, 2022, 2025). Despite progress, these priorities divert funding and infrastructure away from cancer prevention and screening efforts (Atlas of African Health Statistics 2022, 2025, Sichalwe, 2025).
Low health spending and competing priorities
Health spending in SSA remains low, with most countries allocating less than 5 % of GDP to primary healthcare, the main platform for preventive services such as CCS (World Bank, 2023). Limited investment and competing priorities, particularly the focus on infectious diseases (HIV/AIDS, malaria, tuberculosis) and maternal and child health due to their immediate impact on mortality, have left CCS programs underfunded and understaffed. Consequently, screening coverage remains low at about 10 % in SSA (Atlas of African Health Statistics 2022, 2025, Deaton and Tortora, 2015). Moreover, although healthcare ranks high among public priorities, it is often interpreted by governments as emphasising infectious disease control and maternal health rather than cervical cancer prevention (Simmons, K, 2015).
For instance, in Nigeria, CCS is weakly integrated into primary care and concentrated in tertiary and urban facilities, with limited human resources for VIA, cytology, or HPV testing (Olubodun et al., 2022). In Ghana, uptake remains below 10 %, reflecting inadequate financing, limited organised programmes, and substantial access barriers for rural and low-income women (Asgary et al., 2019, Asgedom et al., 2024). By contrast, South Africa shows higher coverage, with around 50 % of women aged 30–49 ever screened, supported by a national policy and greater investment, although rural and poorer groups remain underserved (Yimer et al., 2021). Benin, Tanzania and several other very low-performing countries, where coverage is 0.5–1 %, rely largely on opportunistic or donor driven initiatives (Asgedom et al., 2024, Sichalwe, 2025). These contrasts highlight the heterogeneity of CCS performance across sub-Saharan Africa, emphasizing the need for context-specific strategies rather than assuming a uniform regional picture.
Health System Challenges and Infrastructure Gaps
Most primary healthcare facilities in SSA lack clean water, sanitation, reliable electricity, and basic medical equipment, limiting the delivery of CCS. The African Development Bank (2022)–(2030) reports that only half of facilities have clean water and sanitation, and just one-third have reliable power, constraining quality preventive care (Bank, 2022).
Awareness and cultural influences
In SSA, healthcare providers often show limited knowledge, attitudes, and practices toward CCS, shaped by awareness and cultural factors. A meta-analysis of 30 studies with over 7500 healthcare workers found that while 68 % were knowledge- able and 55 % had positive attitudes, fewer than 20 % of female providers had ever been screened (Delie et al., 2024). Cultural beliefs, stigma, fear, and modesty during gynaecological exams further hinder screening uptake (Adewumi et al., 2022, Delie et al., 2024). Limited training and resources reduce providers’ confidence in promoting CCS, underscoring the need for culturally sensitive programs to address misconceptions and improve provider engagement (Anaman-Torgbor et al., 2020, Delie et al., 2024, Sichalwe, 2025).
The qualifications, training, and availability of health personnel
The qualifications, training, and availability of health personnel have a significant influence on the consistency and quality of cervical cancer screening services in the underserved areas of SSA by influencing several important mechanisms:
Knowledge and attitudes of healthcare providers
In SSA, healthcare providers’ knowledge and attitudes toward CCS vary widely by region, cadre, and training. Knowledge is generally higher among urban physicians and recently trained staff, and lower among rural nurses and clinical officers (Delie et al., 2024). A meta-analysis of 7542 providers found 68 % had adequate knowledge and 55 % had positive attitudes, yet only half knew screening methods, and fewer than 20 % of female providers had ever been screened (Delie et al., 2024). Gaps in knowledge and negative attitudes reduce providers’ ability to counsel patients, perform screenings, and promote uptake. Barriers include unfamiliarity with methods, fear of pain or embarrassment, cultural concerns, and low personal screening rates, which undermine their credibility (Abebaw et al., 2022, Delie et al., 2024). Targeted, culturally sensitive training on cervical cancer, screening guidelines, high-risk groups, and communication skills is essential to improve provider competence, confidence, and community trust, ultimately enhancing screening rates (Abebaw et al., 2022, Delie et al., 2024, Mwalwanda et al., 2024).
Impact of training on clinical competency and self-confidence
Training programs for nurses and frontline health workers in SSA have significantly improved clinical competence in cervical cancer screening, including speculum examination, VIA, and cryotherapy (Beddoe et al., 2017). Experiences from South Africa and Liberia show that such training enhances knowledge, clinical skills, patient communication, and program owner-ship among nurses, leading to increased screening rates and policy support for task-shifting (Beddoe et al., 2017, Brevik et al., 2023). In rural and low-resource settings, trained nurses can lead screening and treatment, improving service access where doctors are scarce. Sustainability relies on ongoing monitoring, regular refresher courses, and supervision to maintain skills, ensure protocol compliance, and uphold quality of care (Asgary et al., 2019). Targeted training thus strengthens workforce capacity, service quality, and program sustainability in SSA.
Awareness of screening guidelines
Healthcare professionals’ awareness of cervical cancer screening guidelines, particularly for high-risk groups such as women living with HIV (WLWH), is often poor. In Tanzania and South Africa, many providers lack knowledge of screening intervals and protocols for WLWH, limiting timely and appropriate screening (Makhubo and Naidoo, 2020, Sichalwe, 2025). Evidence shows that structured training in national and WHO guidelines is crucial for delivering standardised, evidence-based screening, whereas fragmented or absent training results in inconsistent practices and variable outcomes.
Trained staff availability and distribution
Shortages and uneven distribution of trained health staff in resource-limited regions of SSA significantly limit access to CCS. Rural areas often lack providers experienced in VIA, HPV DNA testing, or cytology, reducing timely screening and follow-up (Mantula et al., 2024). Overstretched personnel, tasked with multiple services such as maternal and child health, face high workloads that compromise screening quality and consistency, causing burnout and demotivation (Akinyemiju et al., 2015, Sichalwe, 2025). The concentration of skilled staff in urban areas further exacerbates geographic disparities, forcing rural women to travel long distances or forego care (Sichalwe, 2025). Addressing these human resource gaps is critical for equitable CCS access.
Role modelling and practice among healthcare providers
Female healthcare providers’ own CCS behaviour strongly influences their ability to encourage patients. Low screening rates among providers often reflect gaps in knowledge and attitudes, undermining community trust in screening programs (Adedimeji et al., 2021). Evidence shows that providers who have undergone screening themselves are more credible and enthusiastic advocates, leading to higher patient compliance (Akinyemiju et al., 2015, Makhubo and Naidoo, 2020, Mwalwanda et al., 2024). Effective provider-patient communication, including addressing patient barriers, explaining procedures, and demonstrating encouragement, further increases uptake (Abebaw et al., 2022, Delie et al., 2024). Interventions that enhance providers’ knowledge, personal screening behaviour, and communication skills, such as decision-aid counselling, are essential to strengthen CCS program effectiveness, particularly in low-resource SSA settings (Malekzadeh et al., 2022).
Artificial intelligence-powered solutions for CCS in SSA
Artificial intelligence (AI) provides scalable, cost-effective solutions to CCS challenges in SSA, including shortages of trained staff, laboratories, and infrastructure. Tools like CerviCARE AI allow frontline health workers in rural areas to interpret cervicography images without specialist colposcopists (Sachdeva et al., 2024). In Kenya and other East African countries, deep-learning digital cytology systems scan and analyse Pap smears via cloud-based AI, enabling point-of-care diagnostics (Holmström et al., 2021). The IARC battery-powered AI tool has been piloted in Zimbabwe to triage HPV-positive women offline, while low-cost AI-based automated microscopy platforms achieve over 90 % sensitivity in detecting cervical abnormalities at under USD 500 per unit (IARC, 2024). These innovations can expand access, improve diagnostic accuracy, reduce geographic disparities, and strengthen cervical cancer prevention, supporting WHO’s call for innovative screening and advancing universal health coverage in SSA (Chongsuwat et al., 2023).
Availability and functionality of key screening equipment in CCS programs
Cervical cancer screening uptake in SSA is extremely low, with pooled rates around 12.87 % (Yimer et al., 2021), despite the high disease burden. A key factor is the lack of functional screening equipment, including speculums, acetic acid, cryotherapy machines, and HPV DNA testing kits (Beddoe et al., 2017, Brevik et al., 2023, Burt et al., 2021). In Malawi and rural Ethiopia, women often travel long distances, sometimes repeatedly, because local facilities lack working machines, increasing costs, lost income, and follow-up failure (Cubie and Campbell, 2020, Getachew et al., 2019). Shortfalls also include consumables, maintenance systems, and reliable power, limiting even available equipment (Bank, 2022). Poor referral systems and limited laboratory capacity further impede continuity of care.
Impact of equipment availability on screening precision and participation
The lack of functional equipment, including speculums, acetic acid for VIA, cryotherapy machines, and HPV DNA test kits, undermines the accuracy, credibility, and uptake of CCS in SSA (Delie et al., 2024, Fokom-Domgue et al., 2015). Equipment shortages or malfunctions frustrate providers, compromise sample quality, and increase the risk of missed or incorrect diagnoses. Limited access to advanced technologies, such as HPV DNA testing, reduces adherence to evidence-based protocols and reinforces urban–rural disparities (Black and Richmond, 2018). Frequent stock-outs and weak supply chains disrupt services and lower coverage, contributing to the region’s low screening uptake of around 12.9 % (Yimer et al., 2021). In Nigeria, equipment and supply shortages have caused frequent appointment cancellations (Olubodun et al., 2022), while in Kenya, inconsistent availability of screening apparatuses has limited service reliability and reduced participation (Wexler et al., 2025).
Community trust and provider confidence
Access to functional screening equipment enhances healthcare providers’ confidence in delivering CCS, enabling them to better inform and motivate women, which increases uptake (Delie et al., 2024, Dzinamarira et al., 2023). Conversely, equipment shortages or failures reduce provider morale, diminish enthusiasm for promoting screening, and weaken community trust and participation (Yimer et al., 2021). As role models, providers’ knowledge, attitudes, and behaviours strongly influence public perceptions and willingness to engage with screening programs (Delie et al., 2024).
Discussion
Cervical cancer screening coverage in SSA remains very low, often below 20 %, reflecting limited access to health facilities, inadequate infrastructure, and socioeconomic barriers. A review of 57 countries reported a mean coverage of only 19 % in LMICs, compared to 63 % in HICs (Gakidou et al., 2008). In SSA, geographic remoteness, shortages of trained personnel, and lack of equipment further restrict screening services, contributing to late diagnosis and high mortality (Yimer et al., 2021). In contrast, HICs and some Asian nations achieve coverage above 70 % through structured, publicly funded programs with systematic invitations, advanced laboratory facilities, and effective follow-up systems (Bruni et al., 2022, Sharma et al., 2023). These programs have significantly reduced cervical cancer incidence and mortality over the past decades.
Middle-income countries like Brazil and Thailand achieve 40–70 % cervical cancer screening coverage by integrating services into primary healthcare, using HPV DNA testing, and employing mobile clinics and community outreach (Bruni et al., 2022, Gakidou et al., 2008). In contrast, SSA has low coverage due to limited infrastructure, socio- economic inequalities, and competing health priorities, with urban and wealthier women more likely to be screened than rural or poorer women (Gakidou et al., 2008). Strategies such as task shifting, community mobilization, eHealth, integration into maternal and HIV services, and leveraging health data systems can improve access and coverage, providing sustainable, evidence-based solutions for SSA (Sharma et al., 2023).
Evidence from LMICs outside Africa shows that healthcare providers’ knowledge and attitudes significantly influence the success of cervical cancer screening programs. Systematic reviews indicate that comprehensive VIA training improves providers’ knowledge, attitudes, and patient trust, leading to higher screening uptake (Brevik et al., 2023). In South Africa and Grenada, nurse training enhanced clinical proficiency, provider empowerment, and ownership of screening activities, supporting long-term service delivery (Beddoe et al., 2017). However, gaps remain in counselling skills and quality assessment, which are essential for patient education and program effectiveness (Brevik et al., 2023).
Hands on workshops combining lectures with practical skill stations in LMICs like Malawi, Nepal, and Mozambique have been shown to boost provider competency and confidence in VIA, colposcopy, biopsy, and treatment procedures such as LEEP and thermal ablation (Phoolcharoen et al., 2022). Post-training assessments report 60–76 % of participants feeling more confident, correlating with improved screening quality and coverage (Adewumi et al., 2022, Phoolcharoen et al., 2022). Incorporating guideline training into curricula, reinforced by supervision and refresher courses, is critical to address limited awareness and adherence in SSA, particularly among high-risk populations like women living with HIV (Phoolcharoen et al., 2022).
Task shifting, allowing nurses and midwives to conduct screening and treatment, has successfully expanded the workforce and coverage outside Africa (Phoolcharoen et al., 2022). Mobile training and regional workshops in countries like Nepal and El Salvador have increased the number of trained providers in rural areas (Beddoe et al., 2017, Phoolcharoen et al., 2022). These approaches reduce access inequalities and offer scalable models for resource-poor settings. On-the-job training, peer support, and quality assurance improve provider motivation and service quality (Beddoe et al., 2017, Brevik et al., 2023). VIA training that emphasises client counselling and quality monitoring, often overlooked, enhances screening uptake and patient satisfaction. Evidence from non SSA LMICs also shows that structured training, guideline use, task-shifting, and supervision boost healthcare workers’ skills and confidence, increasing cervical cancer screening coverage (Brevik et al., 2023, Phoolcharoen et al., 2022). Decentralising screening to nurses and community health workers, supported by mentorship and refresher training, can expand rural access and strengthen prevention programs in SSA.
In SSA, the availability and functionality of screening equipment are crucial for effective cervical cancer programs. Many facilities lack essential tools such as colposcopes, cryotherapy or thermal ablation devices, and HPV testing kits, limiting same-day treatment and increasing loss to follow-up (Beddoe et al., 2017, Brevik et al., 2023, Burt et al., 2021). Insufficient equipment and trained personnel reduce screening accuracy, delay treatment, and undermine women’s confidence in services (Stuart and and D’Lima, 2022). In contrast, well-resourced programs in high- and some middle income countries use reliable infrastructure, skilled staff, and quality assurance systems. Innovations such as HPV-based primary screening, self-sampling, and mobile clinics, implemented in Brazil, Thailand, and Western nations, have expanded coverage, improved treatment timeliness, and reduced cervical cancer incidence (Chuang et al., 2021, Tools, 2024). For SSA, investing in functional equipment, workforce training, and efficient service delivery is essential to improve screening quality, access, and follow-up, thereby reducing cervical cancer burden and mortality.
Key determinants for high-quality and high-uptake CCS programs in SSA
Across the reviewed studies, successful CCS programs in low-resource SSA settings consistently shared a combination of effective intervention components, enabling contextual factors, and transferable implementation features. Core intervention components associated with improved screening uptake and quality included:
(i) Community-based health education and mobilisation to address low awareness, stigma, and misconceptions;
(ii) Task-shifting of screening and treatment services to trained nurses and midwives, particularly in rural and primary healthcare settings;
(iii) Integration of CCS into existing maternal, reproductive, and HIV services to leverage established care platforms and increase contact opportunities;
(iv) Use of low-cost and feasible screening approaches such as VIA, HPV DNA testing, and HPV self-sampling; and
(v) Mobile clinics and outreach initiatives to overcome geographic and transport barriers for underserved populations.
Key contextual enablers that supported successful implementation were
(I) Sustained governmental and NGO commitment, including policy support and financing;
(ii) Reliable supply chains for screening consumables, equipment, and treatment devices;
(iii) Continuous training, supportive supervision, and refresher courses to maintain provider competence and confidence;
(iv) Functional data collection, monitoring, and referral systems to ensure service continuity and quality assurance; and
(v) Community engagement strategies that fostered trust and acceptability of screening services.
Commonalities across high-performing programs highlighted several transferable elements for scale-up
Decentralisation of services to primary healthcare facilities, empowerment of frontline health workers through task-shifting, consistent service availability, integration within existing health systems, and adaptability to local sociocultural and health system contexts. Programs that combined these elements demonstrated higher screening coverage, improved follow-up, and greater sustainability.
Improving CCS uptake in SSA requires not isolated interventions but integrated, system-level strategies that align service delivery models with local capacity and community needs. These convergent determinants provide clear, evidence- based guidance for policymakers and implementers seeking to scale up effective and equitable cervical cancer screening programs in similar low-resource settings.
Limitations
A limitation of this study is that it relied exclusively on published literature and selected grey sources, which may have introduced publication bias and limited the comprehensiveness of available data. Additionally, variations in study design, settings, and reporting across included studies may affect the generalizability of the findings. Finally, some contextual factors specific to individual countries may not have been fully captured, limiting the ability to draw nuanced conclusions for all sub-Saharan African settings.
Conclusion
Advancing CCS in SSA requires a coordinated, system-level approach that strengthens healthcare infrastructure, builds workforce capacity, and ensures functional equipment. Sustainable improvements depend on political commitment, adequate financing, integration into existing health platforms, continuous provider support, and community engagement to address social and cultural barriers. Key strategies include integrating VIA and HPV DNA testing into maternal, reproductive, and HIV services, expanding mobile and community-based outreach, improving referral systems with digital tools, implementing culturally sensitive education campaigns, and leveraging AI-powered diagnostics in rural facilities to promote equitable access and accelerate progress toward cervical cancer elimination.
Funding statement
This study received no external funding.
CRediT authorship contribution statement
Magnus Michael Sichalwe: Writing – review & editing, Writing – original draft, Visualization, Supervision, Resources, Project administration, Methodology, Investigation, Funding acquisition, Formal analysis, Data curation, Conceptualization. Abdul Basit: Writing – review & editing, Writing – original draft, Validation, Methodology, Formal analysis. Attiq Ur Rehman: Writing – review & editing, Writing – original draft, Validation, Methodology. Phephile Patience Sifundza: Methodology, Writing – original draft, Writing – review & editing. Grace Tavengana: Writing – review & editing, Writing – original draft, Validation, Methodology. Manas Ranjan Behera: Writing – review & editing, Writing – original draft, Validation, Methodology. Muskan Fatima: Methodology, Resources, Software, Writing – original draft, Writing – review & editing.
Declaration of Competing Interest
The authors declare that they have no known financial or personal conflicts of interest that could have influenced the work reported in this manuscript. This study was conducted independently, without any form of commercial sponsorship, institutional bias, or financial incentive. The research, analysis, interpretation of data, and writing of the manuscript were carried out solely to advance scientific knowledge and public health practice related to cervical cancer screening in low-resource settings.
All authors contributed substantially to the conception and design of the review, data collection, analysis, and interpretation, as well as manuscript drafting and critical revisions for intellectual content. Each author has read and approved the final version of the manuscript and agrees to be accountable for all aspects of the work, ensuring that questions related to the accuracy or integrity of any part of the paper are appropriately investigated and resolved.
The authors further affirm that the review was conducted in adherence to the ethical principles of transparency, integrity, and academic honesty. No part of this work has been previously published or is under consideration for publication elsewhere. This research was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to ensure methodological rigor and reliability.
Acknowledgement
We gratefully acknowledge the authors of the studies included in this review, whose work provided valuable insights and evidence that contributed to the development of this manuscript. Their contributions to advancing research on cervical cancer screening in low-resource settings are deeply appreciated.
References
Abebaw et al., 2022 E. Abebaw, M. Tesfa, W. Gezimu, F. Bekele, A. Duguma Female healthcare providers’ knowledge, attitude, and practice towards cervical cancer screening and associated factors in public hospitals of Northwest Ethiopia. SAGE Open Med., 10 (2022), Article 20503121221095931, 10.1177/ 20503121221095931
Adedimeji et al., 2021A. Adedimeji, R. Ajeh, A. Pierz, R. Nkeng, J. Ndenkeh Jr., N. Fuhngwa, D. Nsame, M. Nji, A. Dzudie, K.M. Anastos, P.E. Castle Challenges and opportunities associated with cervical cancer screening programs in a low income, high HIV prevalence context. BMC Women’S. Health, 21 (2021), p. 74, 10.1186/s12905-021-01211-w
Adewumi et al., 2022 K. Adewumi, H. Nishimura, S.Y. Oketch, P. Adsul, M. Huchko. Barriers and Facilitators to Cervical Cancer Screening in Western Kenya: A Qualitative Study. Journal Cancer Education Official Journal American Association Cancer Education, 37 (4) (2022), pp. 1122-1128, 10.1007/s13187-020-01928-6
Akinyemiju et al., 2015 T.F. Akinyemiju, J.A. McDonald, P.M. Lantz. Health care access dimensions and cervical cancer screening in South Africa: Analysis of the world health survey. BMC Public Health, 15 (1) (2015), p.382, 10.1186/s12889-015-1686-5
Anaman-Torgbor et al., 2020 J. Anaman-Torgbor, S.K. Angmorterh, D. Dordunoo, E.K. Ofori. Cervical cancer screening behaviours and challenges: A sub-Saharan Africa perspective. Pan Afr. Med. J., 36 (2020), p. 97, 10.11604/pamj.2020.36.97.19071
Asgary et al., 2019 R. Asgary, H. Cole, P. Adongo, A. Nwameme, E. Maya, A. Adu-Amankwah, H. Barnett, R. Adanu. Acceptability and implementation challenges of smartphone-based training of community health nurses for visual inspection with acetic acid in Ghana: mHealth and cervical cancer screening. BMJ Open, 9 (7) (2019), Article e030 528, 10.1136/bmjopen-2019-030528
Asgedom et al., 2024 Y.S. Asgedom, G.A. Kassie, A. Habte, D.B. Ketema, F.M. Aragaw. Socioeconomic inequality in cervical cancer screening uptake among women in sub-Saharan Africa: A decomposition analysis of Demographic and Health Survey data
BMJ Open, 14 (12) (2024), Article e088753, 10.1136/bmjopen-2024-088753
Atlas of African Health Statistics 2022, 2025. Atlas of African Health Statistics 2022: Health situation analysis of the WHO African Region | WHO | Regional Office for Africa. (2025, June 4).〈https://www.afro.wh o.int/ publications/atlas-african-health-statistics-2022-health-situation-analysis-who-african-region-1〉.
Ba et al., 2021 D.M. Ba, P. Ssentongo, J. Musa, E. Agbese, B. Diakite, C.B. Traore, S. Wang, M. Maiga. Prevalence and Determinants of Cervical Cancer Screening in Five Sub-Saharan African Countries: A Population-Based Study. Cancer Epidemiol., 72 (2021), Article 101930, 10.1016/j.canep.2021. 101930
Bank, 2022 Bank, A.D. (2022, May 18). Strategy for Quality Health Infrastructure in Africa—2022-2030 [Text]. African Development Bank Group; African Development Bank Group.
〈https://www.afdb.org/en/ documents/strategy-quality-health-infrastructure-africa-2022-2030〉.
Beddoe et al., 2017 A.M. Beddoe, O. Afzal, M. Lieber, W. Jallah, C. McIntosh, P. Dottino. Training health workers to provide cervical cancer screening: comparison of educational strategies in Liberia, South Africa and Grenada. Ann. Glob. Health, 83 (1) (2017), p. 53, 10.1016/j.aogh.2017.03.117
Binagwaho et al., 2012 A. Binagwaho, C.M. Wagner, M. Gatera, C. Karema, C.T. Nutt, F. Ngabo. Achieving high coverage in Rwanda’s national human papillomavirus vaccination programme. Bull. World Health Organ., 90 (8) (2012), pp. 623-628, 10.2471/BLT. 11.097253
Black and Richmond, 2018 E. Black, R. Richmond. Prevention of cervical cancer in Sub-Saharan Africa: the advantages and Challenges of HPV Vaccination Article 3 Vaccines, 6 (3) (2018), 10.3390 / vaccines6030061
Brevik et al., 2023 T.B. Brevik, L.R. da Matta Calegari, I. Mosquera Metcalfe, P. Laake, M. Maza, P. Basu, A. Todd, A.L. Carvalho. Training health care providers to administer VIA as a screening test for cervical cancer: A systematic review of essential training components. BMC Med. Educ., 23 (2023), p. 712, 10.1186/s12909-023-04711-5
Bruni et al., 2022 L. Bruni, B. Serrano, E. Roura, L. Alemany, M. Cowan, R. Herrero, M. Poljak, R. Murillo, N. Broutet, L.M. Riley, S. de Sanjose. Cervical cancer screening programmes and age-specific coverage estimates for 202 countries and territories worldwide: A review and synthetic analysis. Lancet Glob. Health, 10 (8) (2022), pp. e1115-e1127, 10.1016/S2 214-109X (22)00241-8
Burt et al., 2021 L.M. Burt, M. McCormak, F. Lecuru, D.M. Kanyike, M. Bvochora-Nsingo, N. Ndlovu, A.A. Scott, R.I. Anorlu, V. Sharma, M. Plante, C. Nyongesa, W. Tigeneh, N. Fakie, G. Suneja, D.K. Gaffney. Cervix cancer in sub-saharan africa: an assessment of cervical cancer management. JCO Glob. Oncol., 7 (2021), pp.173-182,10.1200/GO.20.00079
Campos et al., 2024 N.G. Campos, D.R. Lowy, S. de Sanjosé, M. Schiffman. A cervical cancer control strategy for lower-resource settings: Interventions to complement one-dose HPV vaccination. J. Natl. Cancer Inst. Monogr., 2024 (67) (2024), pp. 417-423, 10.109 3/jncimonographs/lgae040
Chongsuwat et al., 2023 T. Chongsuwat, C. Wang, Y. Sohn, K. Klump. Digital cervicography for cervical cancer screening in low-resource settings: A scoping review. Gynecol. Oncol. Rep., 45 (2023), Article 101130, 10.1016/j.gore.2022.101 130.
Chuang et al., 2021 L. Chuang, N. Rainville, M. Byrne, T. Randall, K. Schmeler. Cervical cancer screening and treatment capacity: A survey of members of the African Organisation for Research and Training in Cancer (AORTIC). Gynecol. Oncol. Rep., 38 (2021), Article 100874, 10.1016/j.gore. 2021.1008 74
Cubie and Campbell, 2020 H.A. Cubie, C. Campbell. Cervical cancer screening – The challenges of complete pathways of care in low-income countries: Focus on Malawi Women’S. Health (Lond. Engl. ), 16 (2020), Article 1745506520 914804,10.1177/ 1745506520 914804
Deaton and Tortora, 2015 A.S. Deaton, R. Tortora. People In Sub-Saharan Africa Rate Their Health And Health Care Among Lowest In World. Health Aff. (Proj. Hope), 34 (3) (2015), pp. 519-527, 10.1377/hlthaff.2014.0798
Delie et al., 2024 A.M. Delie, E.K. Bogale, T.F. Anagaw, M.G. Tiruneh, E.T. Fenta, D. Endeshaw, H.B. Eshetu, O. Adal, A.A. Tareke, N. Kebede. Healthcare providers’ knowledge, attitude, and practice towards cervical cancer screening in Sub-Saharan Africa: Systematic review and meta-analysis. Front. Oncol., 14 (2024), Article 1436095, 10.3389/fonc.2024. 1436095
Dzinamarira et al., 2023 T. Dzinamarira, E. Moyo, M. Dzobo, E. Mbunge, G. Murewanhema. Cervical cancer in sub-Saharan Africa: An urgent call for improving accessibility and use of preventive services. Int. J. Gynecol. Cancer, 33 (4) (2023), pp. 592-597, 10.1136/ijgc-2022-003957
Fokom-Domgue et al., 2015 Fokom-Domgue, J., Combescure, C., Fokom-Defo, V., Tebeu, P.M., Vassilakos, P., Kengne, A.P., & Petignat, P. (2015). Performance of alternative strategies for primary cervical cancer screening in sub-Saharan Africa: Systematic review and meta-analysis of diagnostic test accuracy studies. https://doi.org/10.1136/bmj.h3084.
Gakidou et al., 2008 E. Gakidou, S. Nordhagen, Z. Obermeyer. Coverage of cervical cancer screening in 57 countries: Low average levels and large inequalities. PLoS Med., 5 (6) (2008), Article e132, 10.1371/journal.pmed. 0050132
Getachew et al., 2019 S. Getachew, E. Getachew, M. Gizaw, W. Ayele, A. Addissie, E.J. Kantelhardt. Cervical cancer screening knowledge and barriers among women in Addis Ababa, Ethiopia. PloS One, 14 (5) (2019), Article e0216522, 10.1371/journal. pone.0216522
Health system building blocks, 2023 Health system building blocks. (2023). Retrieved March 3, 2025, from 〈https://extranet.who.int/ nhptool/BuildingBlock.aspx〉 Healthcare Infrastructure: Meaning, defination, significance, challenges | Enterprise Wired. (2023, November5). 〈https://enterprisewired.com/ meaning-of-healthcare-infrastructure/〉.
Holmström et al., 2021 O. Holmström, N. Linder, H. Kaingu, N. Mbuuko, J. Mbete, F. Kinyua, S. Törnquist, M. Muinde, L. Krogerus, M. Lundin, V. Diwan, J. Lundin. Point-of-Care Digital Cytology With Artificial Intelligence for Cervical Cancer Screening in a Resource-Limited Setting. JAMA Netw. Open, 4 (3) (2021), Article e211740, 10.1001 /jamanetwork open.2021.1740
IARC, 2024 IARC-developed AI outperforms standard tests in a leap towards global health equity. (2024). Retrieved August 5, 2025, from https://www.iarc.who. int/news-events/iarc-developed-ai-out performs-standard-tests-in-a-leap-towards-global-health-equity.
Makhubo and Naidoo, 2020 M.T. Makhubo, T.D. Naidoo. Healthcare worker compliance with cervical cancer screening guidelines. An audit at district and regional level of care in the Pietermaritzburg Metropolitan area of KwaZulu-Natal South. Afr. J. HIV Med., 21 (1) (2020), p. 1104, 10.4102/sajhivmed. v21i1.1 104
Malekzadeh et al., 2022E. Malekzadeh, R. Nourizadeh, A. Farshbaf-Khalili, E. Mehrabi, S. Hakimi. The effect of decision-aid-based counseling on cervical cancer screening behavior among women: An interventional study. J. Educ. Health Promot., 11 (1) (2022), p. 205, 10.4103/jehp.jehp _714_21
Mantula et al., 2024 F. Mantula, Y. Toefy, V. Sewram. Barriers to cervical cancer screening in Africa: A systematic review BMC Public Health, 24 (2024), p. 525, 10.1186/s12889-024-17842-1
Mwalwanda et al., 2024 A. Mwalwanda, E. Chavura, M.R.O. Chisale, B.C. Mbakaya. Cervical cancer screening among female health workers: Evidence from a secondary health facility in Northern Malawi. Prev. Med. Rep., 37 (2024), Article 102581, 10.1016/j.pmedr.2023.10 2581
NCI, 2022 NCI. Cervical Cancer Causes, Risk Factors, and Prevention. (nciglobal, ncienterprise). (2022, October 13). [pdqCancerInfo Summary]. 〈https://www.cancer. gov/types/cervical/causes-risk-prevention〉.
Olubodun et al., 2022 T. Olubodun, M.R. Balogun, A.K. Odeyemi, O.O. Odukoya, A.O. Ogunyemi, O.J. Kanma-Okafor, I.P. Okafor, A.B. Olubodun, O.O.P. Ogundele, B. Ogunnowo, A. Osibogun. Barriers and recommendations for a cervical cancer screening program among women in low-resource settings in Lagos Nigeria: A qualitative study. BMC Public Health, 22 (1) (2022), p. 1906, 10.1186/s12889-022-14314-2
Page et al., 2021 M.J. Page, J.E. McKenzie, P.M. Bossuyt, I. Boutron, T.C. Hoffmann, C.D. Mulrow, L. Shamseer, J.M. Tetzlaff, E.A. Akl, S.E. Brennan, R. Chou, J. Glanville, J.M. Grimshaw, A. Hróbjartsson, M.M. Lalu, T. Li, E.W. Loder, E. Mayo-Wilson, S. McDonald, …, D. Moher. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews BMJ (Clin. Res. Ed. ), 372 (2021), p. n71, 10.1136/bmj.n71
Petersen et al., 2022 Z. Petersen, A. Jaca, T.G. Ginindza, G. Maseko, S. Takatshana, P. Ndlovu, N. Zondi, N. Zungu, C. Varghese, G. Hunting, G. Parham, P. Simelela, S. Moyo. Barriers to uptake of cervical cancer screening services in low-and-middle-income countries: A systematic review BMC Women’S. Health, 22 (1) (2022), p. 486, 10.1186/s12905-022-02043-y
Phoolcharoen et al., 2022 N. Phoolcharoen, M.L. Varon, E. Baker, S. Parra, J. Carns, K. Cherry, C. Smith, T. Sonka, K. Doughtie, C. Lorenzoni, R. Richards-Kortum, K. Schmeler, M.P. Salcedo Hands-On Training Courses for Cervical Cancer Screening, Diagnosis, and Treatment Procedures in Low- and Middle-Income Countries. JCO Glob. Oncol. (8) (2022), Article e2100214, 10.1200/GO.21.00214
ROCHE, 2025 ROCHE. The economic imperative of cervical cancer elimination: A call to action for healthcare leaders. (2025, September 29). 〈https://www.roche.com/ stories/economic-imperative-of-cervical-cancer-elimination〉.
Sachdeva et al., 2024 M. Sachdeva, A.M. Datchoua, V.F. Yakam, B. Kenfack, M. Jonnalagedda-Cattin, J.-P. Thiran, P. Petignat, N.C. Schmidt. Acceptability of artificial intelligence for cervical cancer screening in Dschang, Cameroon: A qualitative study on patient perspectives. Reprod. Health, 21 (2024), p. 92, 10.1186/s12978-024-01828-8
Sahasrabuddhe et al., 2012 V.V. Sahasrabuddhe, G.P. Parham, M.H. Mwanahamuntu, S.H. Vermund. Cervical Cancer Prevention in Low- and Middle-Income Countries: Feasible, Affordable, Essential. Cancer Prev. Res., 5 (1) (2012), pp. 11-17, 10.1158/1940-6207.CAPR -11-0540
Sharma et al., 2023 J. Sharma, M. Yennapu, Y. Priyanka. Screening guidelines and programs for cervical cancer control in countries of different economic groups: a narrative review. Cureus, 15 (6) (2023), Article e41098, 10.7759/cureus.41098
Sichalwe, 2025 M.M. Sichalwe. Barriers and Facilitators of Cervical Cancer Screening among Tanzanian Women: A Systematic Review. Article 1. J. Cerv. Cancer Res., 7 (1) (2025), 10.36959/749/527
Simmons and K, 2015 R.W. Simmons, K. Health Care, Education Are Top Priorities in Sub-Saharan Africa September 16 Pew Res. Cent. (2015). https://www.pewresearch.org/global/2015/09/16/ health-care-education-are-top-priorities-in-sub-saharan-africa/〉
Simms et al., 2023 K.T. Simms, A. Keane, D.T.N. Nguyen, M. Caruana, M.T. Hall, G. Lui, C. Gauvreau, O. Demke, M. Arbyn, P. Basu, N. Wentzensen, B. Lauby-Secretan, A. Ilbawi, R. Hutubessy, M. Almonte, S. De Sanjosé, H. Kelly, S. Dalal, L.O. Eckert, …, K. Canfell. Benefits, harms and cost-effectiveness of cervical screening, triage and treatment strategies for women in the general population. Nat. Med., 29 (12) (2023), pp. 3050-3058, 10.1038/s41591-023-02600-4
Singh et al., 2023 D. Singh, J. Vignat, V. Lorenzoni, M. Eslahi, O. Ginsburg, B. Lauby-Secretan, M. Arbyn, P. Basu, F. Bray, S. Vaccarella. Global estimates of incidence and mortality of cervical cancer in 2020: A baseline analysis of the WHO Global Cervical Cancer Elimination Initiative. Lancet Glob. Health, 11 (2) (2023), pp. e197-e206, 10.1016/S2214-109X (22)00501-0
Stuart and D’Lima, 2022 G. Stuart, D. D’Lima. Perceived barriers and facilitators to attendance for cervical cancer screening in EU member states: A systematic review and synthesis using the Theoretical Domains Framework. Psychol. Health, 37 (3) (2022), pp. 279-330, 10.1080/088704 46.2021. 1918690
Sung et al., 2021 H. Sung, J. Ferlay, R.L. Siegel, M. Laversanne, I. Soerjomataram, A. Jemal, F. Bray. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer Journal Clinicians, 71 (3) (2021), pp. 209-249, 10.33 22/caac. 21660
Tools, 2024 Tools, S. (2024). HPV World. HPV World. Retrieved June 22, 2025, from 〈https://www.hpvworld .com/〉.
Wexler et al., 2025 C. Wexler, M. Maloba, N. Mabachi, N. Maosa, S. Babu, V.S. Staggs, S. Mokua, K. Goggin, S. Finocchario-Kessler. Availability and Uptake of Cervical Cancer Screening and Treatment Services at 19 Kenyan Health Facilities: A Brief Report
JCO Glob. Oncol. (11) (2025), Article e2400255, 10.1200/GO-24-00255
WHO, 2024 WHO. Cervical Cancer Elimination Initiative. (2024). Retrieved December 21, 2024, from 〈https://www.who.int/ initiatives/cervical-cancer-elimination-initiative〉.
World Bank, 2023 World Bank. Three strategies to unlock the potential of primary health care in Sub-Saharan Africa World Bank Blogs (2023). https://blogs.worldbank.org/en/health/ three-strategies-unlock-potential-primary-health-care-sub-saharan-africa〉
Yang et al., 2023 L. Yang, M.-C. Boily, M.M. Rönn, D. Obiri-Yeboah, I. Morhason-Bello, N. Meda, O. Lompo, P. Mayaud, M. Pickles, M. Brisson, C. Hodgins, S. Delany-Moretlwe, M. Maheu-Giroux. Regional and country-level trends in cervical cancer screening coverage in sub-Saharan Africa: A systematic analysis of population-based surveys (2000–2020)
PLOS Med., 20 (1) (2023), Article e1004143, 10.1371/journal. pmed. 1004143
Yimer et al., 2021 Yimer, N.B., Mohammed, M.A., Solomon, K., Tadese, M., Grutzmacher, S., Meikena, H.K., Alemnew, B., Sharew, N.T., & Habtewold, T.D. (2021). Cervical cancer screening uptake in Sub-Saharan Africa: A systematic review and meta-analysis (p. 2020.12.26.202488 64). medRxiv. https://doi.org/10. 1101/2020.12.26.20248864.