

Joseph Weddell, Wendan Shi, Julie Redfern, Thomas Buckley, Robyn Gallagher
Abstract
Aims
The primary aim of this study was to investigate the effect of peer support interventions on psychosocial outcomes, self-management behaviours, and readmissions among people with coronary heart disease (CHD). The secondary aim was to characterize the peer support strategies being tested, including the intervention initiation, method, dose, timing, format, and content, and the characteristics and training of the peers providing the intervention.
Methods and Results
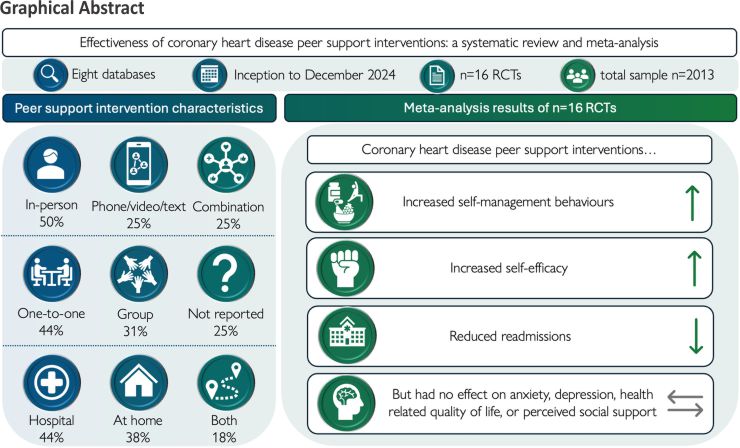
Systematic review and meta-analysis [MEDLINE, Embase, PsycINFO, CINAHL, Scopus, PubMed (non-MEDLINE), Web of Science, and Cochrane Central Register] and risk of bias appraisal were conducted on the above outcomes according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist and Cochrane Collaboration guidelines. Meta-analysis was undertaken in RevMan5.4 using the inverse variance method and random effects model. Intervention components and outcomes unsuitable for meta-analysis were narratively synthesized. Sixteen randomized controlled trials (n = 2013) were included. Peer support had no effect on anxiety [standardized mean difference (SMD) −0.73, 95% confidence interval (CI) −1.57, 0.10], depression (SMD −0.09, 95% CI −0.25, 0.06), health-related quality of life (SMD −0.38, 95% CI −1.84, 1.08), or perceived social support (SMD −0.05, 95% CI −0.31, 0.21). However, peer support interventions significantly improved self-management behaviours (SMD 1.49, 95% CI 0.66, 2.32) and self-efficacy up to 6 months (SMD 0.57, 95% CI 0.37, 0.77) and reduced readmissions (risk ratio 0.25, 95% CI 0.10, 0.60). Self-efficacy remained higher in those receiving peer support at 6–12 months post-intervention (SMD 0.67, 95% CI 0.29, 1.05). The characteristics of peer support interventions were diverse and varied widely, but the most commonly used strategies included in-person (56%), group-based (31%), and experience sharing (44%). Although subgroup analysis was not possible, narrative synthesis indicated that in-person strategies and peer support that was commenced during admission were the most effective for improving outcomes.
Conclusion
Peer support interventions for people with CHD may be used to improve self-management and self-efficacy and reduce readmission risk, but anxiety, depression, health-related quality of life, and social support did not reach statistical significance when meta-analysed. In-person, group-based, and experience sharing were the most common peer support categories, and strategies that were in-person and initiated during admission demonstrated the most consistent improvements across outcomes.
Keywords Psychosocial outcome measures, Self-management, Readmission, Coronary heart disease, Peer group, Peer support, Systematic review, Meta-analyses, Cardiac rehabilitation
Lay Summary
People with coronary heart disease who have received a peer support intervention (support from somebody else with the same condition) demonstrate better heart disease self-management behaviours, have greater confidence to put these behaviours into practice, and are less likely to be readmitted to hospital. No difference was observed in anxiety, depression, health-related quality of life, and perceived social support between those receiving peer support and those receiving routine care. Peer support interventions for coronary heart disease are varied and delivered with many different approaches, and the exact mechanisms behind specific elements of peer support require further investigation.
Introduction
Cardiovascular disease remains a leading cause of death and disability worldwide, and recurrence is common.1 Approximately one in five acute coronary syndrome (ACS) inpatients are readmitted within 1 year of presentation,2 and these recurrences are largely avoidable with secondary prevention strategies and lifestyle changes.3 However, secondary prevention can be challenging to initiate and sustain, as learning multiple new skills for self-management is often necessary, which then must be incorporated into everyday life.4 Coronary heart disease (CHD) diagnosis often results in psychosocial impacts, including anxiety, depression, feelings of isolation, and worsening health-related quality of life (HRQoL), which are often identified as patient-reported outcomes.5–8 Social support is important in addressing adverse CHD outcomes associated with these challenges, such as isolation,9 feelings of hopelessness,10 and depression,11 but is not available to everyone. All of these impacts, including lack of social support, are established risk factors that increase cardiac morbidity and mortality 12 but are also burdensome to patients, make behavioural change more difficult, and limit confidence (self-efficacy) to enact new knowledge into practice.13,14 Secondary prevention behaviours are therefore not always initiated or maintained, for example, with adherence to medication decreasing by 1 year15 and a lack of engagement in physical exercise.16 Cardiac rehabilitation addresses psychosocial issues, promotes self-management behaviours, and provides opportunities for interaction with peers; however, programmes often lack personalization and have poor uptake or issues with access.17 Peer support has been proposed as a potential solution to provide support, address psychosocial issues, and promote secondary prevention efforts.18
Peer support is defined as help, support, or information, substantiated by experiential knowledge, that is shared between people with the same health condition, to help manage that condition.19,20 Peer support is distinct from other forms of social support provided by family, friends, communities, and professionals because the support received and given is grounded in the lived experience of the same condition.20 Peer support interventions can be delivered by a variety of strategies, which can differ by mode of delivery (e.g., in person, telephone, messaging, and combinations), interaction (support groups or one-to-one), timing of initiation (e.g., hospital admission, post-discharge, and combinations), and duration.19,21 Patients with ACS report sharing experiences and discussing health challenges to be more useful with peers than with family or friends, because peers can mutually understand and relate to experiences.22 Numerous benefits of peer support participation have been reported, including normalizing illness experiences, enabling knowledge exchange, increasing motivation, building self-care confidence, benchmarking progress, reducing isolation, fostering shared recovery journeys, and vicarious problem solving.22–25
In chronic conditions, such as cancer, peer support interventions have demonstrated improvements in HRQoL, depression, anxiety, and self-efficacy.21 However, the effects of peer support in CHD populations are less certain. A 2009 systematic review identified six studies of peer support interventions for heart disease [including heart failure, cardiac surgery, and previous myocardial infarction (MI)] and reported improvements in self-efficacy and well-being.26 On the other hand, a 2023 Cochrane review of social network interventions for CHD [including 23/49 (43%) studies with interventions delivered by peers] reported modest improvements in blood pressure and HRQoL but noted the low-quality evidence to be a significant limitation.27 Both reviews included broader definitions of heart disease (not solely CHD) and peers (not solely people with the same condition) and noted high heterogeneity of interventions and variable quality of evidence that made generalizability of results difficult.26,27 To the best of our knowledge, no reviews have been undertaken that investigate the effect of peer support intervention on psychosocial outcomes, self-management behaviours, or readmissions among people with CHD or the individual characteristics of peer support interventions.
Objective
The primary aim of this study was to investigate the effect of peer support interventions on psychosocial outcomes, self-management behaviours, and readmissions among people with CHD. The secondary aim was to characterize the peer support strategies being tested, including the intervention initiation, method, dose, timing, format, and content, and the characteristics and training of the peers providing the intervention.
Methods
Study design and selection criteria
A systematic review and meta-analysis were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (see Supplementary material).28 The review was registered on PROSPERO (CRD42024514564) prior to data extraction commencing. This PROSPERO protocol has since had one minor amendment submitted to include the secondary aims of readmission outcomes and peer support intervention characteristics, which were identified as important considerations after initial PROSPERO registration and study selection.
Studies were eligible for inclusion if (i) participants had a primary diagnosis of CHD, (ii) the peer support intervention [including any context, setting, format, or purpose (e.g. education)] was delivered by a person (or people) with a diagnosis of CHD, to a person (or people) with the same diagnosis, (iii) psychosocial outcomes, self-management behaviour outcomes (i.e. collective secondary prevention behaviours), or readmissions were measured, (iv) a randomized controlled trial (RCT) study design was used, and (v) the comparator arm was usual care (including or excluding cardiac rehabilitation) without peer support. The peer support intervention definition of Thompson et al.19 and the Agency for Clinical Innovation20 was used for this review to emphasize the importance of interaction between people with lived experience of the same condition as a key component of the intervention. We excluded any study that defined peer support as support from healthcare professionals, friends, families, or individuals without CHD. However, studies with peer support interventions, as defined above, but which also included healthcare professionals, family, and friends, were not specifically excluded, proving that the inclusion criteria were met. Published theses were not included as individual studies but were drawn upon if the thesis provided information from a corresponding published article (i.e., refers to the same sample, ethics, and study). Based on the Cochrane Handbook, the decision to include only RCTs was to account for baseline differences between participant characteristics and because statements of cause and effect can be made with higher confidence than with other study designs.29
Search strategy, data sources, and study selection
Eight electronic databases were searched (J.W.) from inception to 15 November 2023, with the search updated on 18 December 2024 prior to manuscript submission: MEDLINE, Embase, and PsycINFO via OVID, CINAHL (Cumulative Index to Nursing & Allied Health Literature) via EBSCO, Scopus, PubMed (non-MEDLINE), Web of Science, and the Cochrane Central Register of Controlled Trials (CENTRAL). The search strategy was developed using the PICOT framework in consultation with an academic liaison librarian, subject headings identified for each database, and free text terms with database-specific syntax compiled (see Supplementary material online, Material S1). The search was constructed from two main concepts: (i) CHD and (ii) peer support interventions. Hand searches using a snowballing technique (manual reference list searching) were utilized after the first round of searching. No filters or limits were applied.
Data extraction
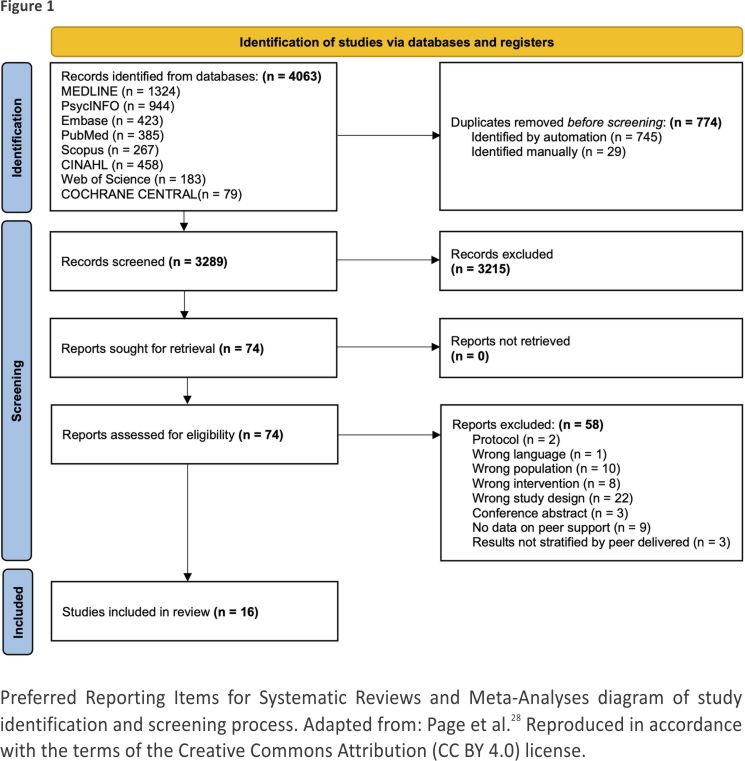
All citations were imported into Zotero 6.0.37 Citation Management Software before being uploaded into Covidence Systematic Review Software for screening and data extraction.30 Duplicates were removed automatically in Covidence and manually were identified. Titles and abstracts were screened independently for eligibility by two investigators (J.W. and W.S.). Articles identified that fulfilled the inclusion criteria above were then obtained in full text and assessed independently for eligibility by both investigators (Figure 1). Disagreements were resolved by discussion between the two investigators, with a third investigator (R.G.) consulted for on-going disputes. The primary investigator (J.W.) performed data extraction and data entry, which was then checked by a second reviewer (W.S.). Microsoft Excel was used for data collection using a form developed prior to extraction. Data extracted included sample size and description, quality appraisal, intervention method of delivery, length of intervention, number of peer support sessions, information regarding who the peers were, and outcomes. The corresponding author of one study31 was contacted to seek further information but did not respond.
All included studies underwent risk of bias appraisal using guidelines in the Cochrane Handbook for Systematic Reviews of Interventions. 32 Risk of bias was independently conducted by two investigators (J.W. and W.S.), with a third investigator for consensus (R.G.) on disagreements. Quality appraisal consisted of sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selecting reporting, and other bias detailed in the handbook. Risk of bias was determined as high, low, or unclear.
Statistical analysis
Statistical analysis was undertaken using RevMan 7.4.1 software for meta-analysis as guided by the Cochrane Handbook.33 Categorical data were reported using frequencies with percentages. Continuous data were assessed for skewedness and reported using means with standard deviations (SD) (normal distribution) or by medians and mode with interquartile range (IQR) (skewed distribution). The effect of CHD peer support interventions on (i) psychosocial outcomes, (ii) outcomes relating to self-management behaviours, and (iii) readmissions was pooled for overall estimate of treatment effect and meta-analysed using the inverse-variance method and a random effects model. Outcomes that occurred singularly (i.e. not across multiple studies), that were reported without means and SD, or that were measured with the use of an unvalidated instrument were unable to be meta-analysed and were therefore narratively synthesized. Outcomes were pooled according to the time at follow-up when data were reported: <6 months or 6–12 months. Standardized mean differences (SMDs) or risk ratios were then used to report outcome variables alongside 95% confidence intervals (CIs), according to continuous or categorical data. Heterogeneity was assessed statistically using I2 and assessed qualitatively by comparing variability in participants, interventions, and outcomes (clinical diversity) and in outcome measurement tools and risk of bias (methodological diversity). Subgroup analysis and funnel plots to assess publication bias were not feasible due to the limited number of studies.33
Results
Identification of relevant articles
A total of 4063 articles were identified, of which 774 were removed as duplicates, and 3289 were then assessed for potential inclusion in title and abstract screening, during which 3215 were excluded (Figure 1). Of the 74 articles assessed during full-text screening, 58 were excluded due to being the wrong study design (n = 22), population (n = 10), or intervention (n = 8), or for not providing (n = 9) or stratifying (n = 3) data on peer support, or for being a protocol (n = 2), conference abstract (n = 3), or article not written in English (n = 1). A total of 16 RCTs were included in the final result (Figure 1).31,34–48
Study characteristics
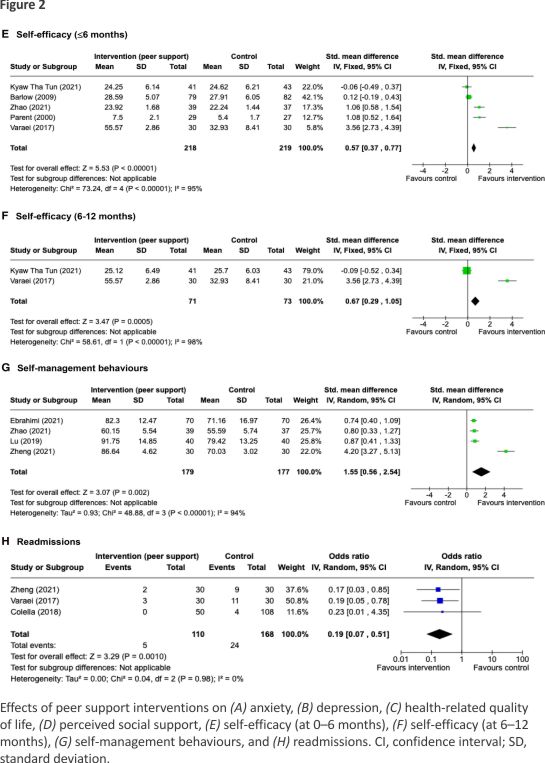
The total sample (n = 2013) was 64% male with a weighted mean age of 57.7 ± 12.3 years. Two studies used an exclusively male sample34,40 and another used an exclusively female sample.38 The sample diagnosis varied across studies including coronary artery bypass graft (CABG) patients (7/16, 44%), first-time MI or CHD admission (5/16, 31%), percutaneous coronary intervention (PCI) patients (3/16, 19%), and women with a CHD diagnosis made in the previous year (1/16, 6%). Cardiac rehabilitation attendance was a pre-requisite for participation in one study (6%), not reported in five studies (31%), not applicable in seven studies due to inpatient study setting (44%), measured as an outcome (enrolment or attendance) in two study (13%), and delivered as a (peer-led) intervention in one study (6%). In the control arm of two studies (13%), participants also attended cardiac rehabilitation on top of usual care. Outcomes were measured with a variety of instruments (Table 1), the score ranges of which are reported in Supplementary material online, Material S2. Outcomes assessed up to 6 months from baseline were pooled for meta-analyses, including anxiety (7 studies, n = 589), depression (6 studies, n = 652), HRQoL (4 studies, n = 313), self-management behaviours (4 studies, n = 356), and self-efficacy (5 studies, n = 437) and for 6–12-month outcomes for self-efficacy (2 studies, n = 144) (Figure 2).
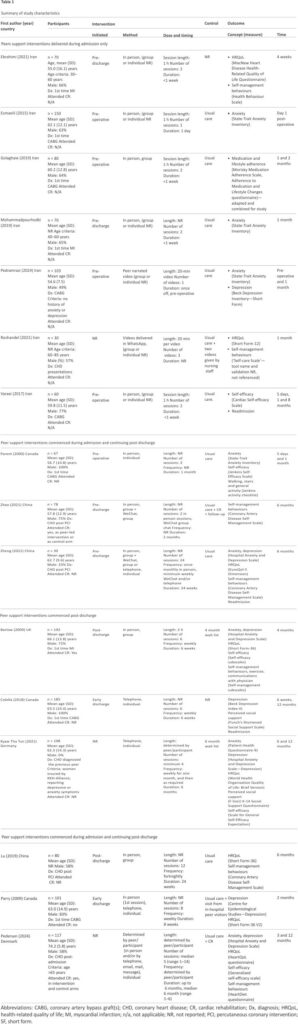
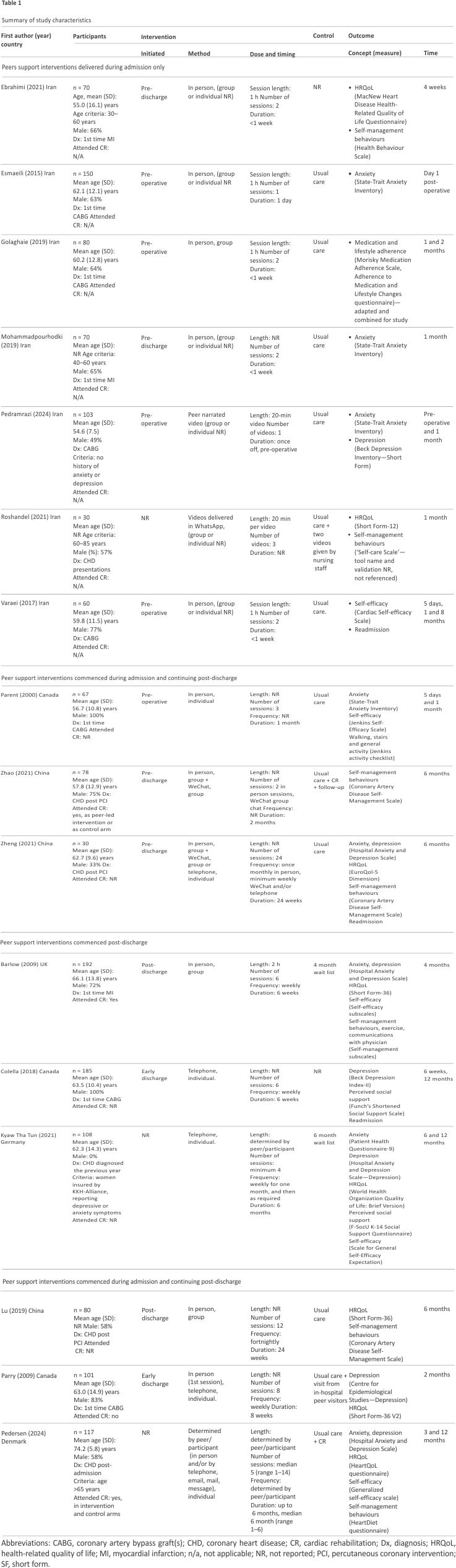
Peer support interventions were initiated pre-CABG (5/16, 31%), pre-discharge (4/16, 25%), at early discharge (3/16, 19%), post-discharge (2/16, 13%), or at a timing that was not reported (2/16, 13%) (Table 1). Peer support interventions were delivered in person (8/16, 50%), in person initially and then remotely [telephone, 1/16, 6%; messaging (i.e. WeChat or WhatsApp) 1/16, 6%; or both 1/16, 6%], entirely remotely (3/16, 19%) via telephone (2/16, 13%), messaging (1/16, 6%), or video (1/16, 6%), or by any of the above formats, as determined by the peer and supporter (1/16, 6%). No peer support interventions were delivered online or via mobile application. Interventions were group (5/16, 31%) or individually based (i.e. one to one; 5/16, 31%), with 6/16 studies (38%) not reporting this information. Sessions lasted for 20 min (2/16, 13%), 1 h (4/16, 25%), 2 h (1/16, 6%), or for a length of time either not reported (7/16, 44%) or determined by the peer and participant (2/16, 13%). The number of sessions ranged from 1 to 24, with a mode of 2 and median of 3 (IQR 4). Sessions continued over the duration of the week of admission (7/16, 44%) or for 4 (2/16, 13%), 6–8 (4/16, 25%), or 24 weeks (3/16, 19%).
Peer supporter selection and training
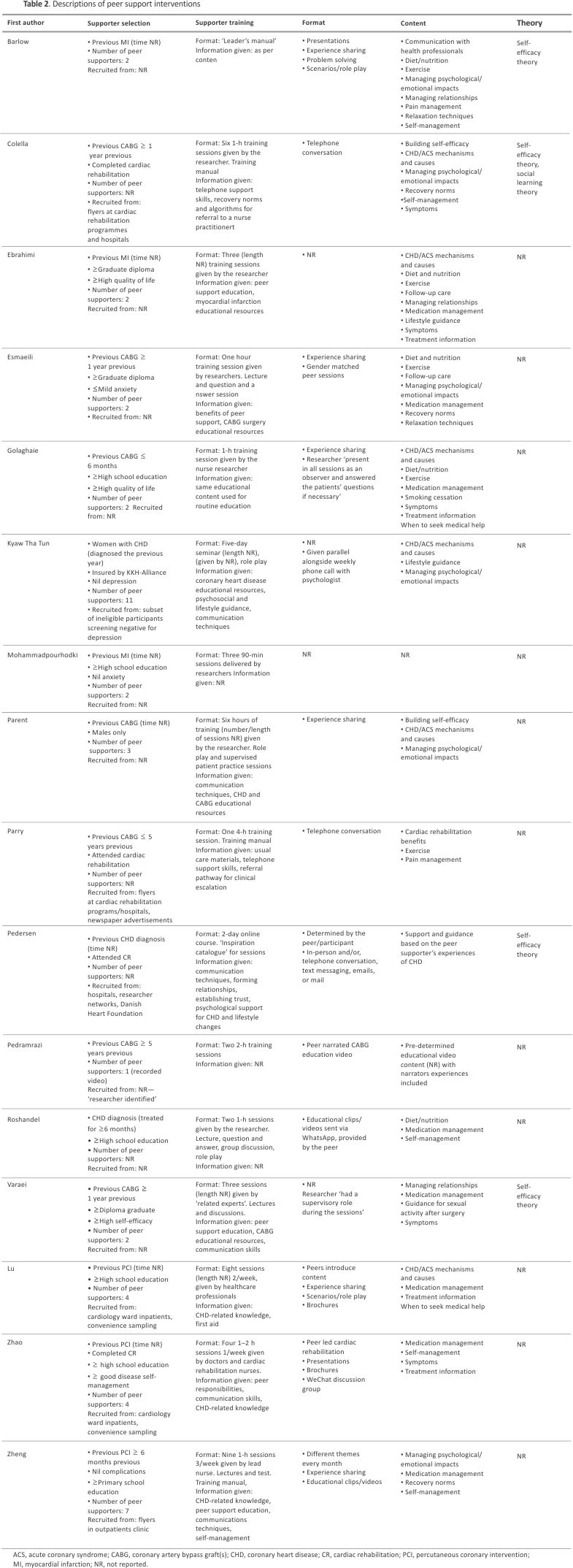
Peer supporters in studies were selected based on having a previous MI (3/16, 19%), CABG (7/16, 44%), PCI (3/16, 19%), or CHD diagnosis (3/16, 19%) (Table 2). The number of peer supporters in each intervention ranged from 1 to 11 (median 2, mode 2, and IQR 2) with 4/16 (25%) studies not reporting how many peers were involved. Specific eligibility criteria for the peer supporters included a minimum amount of education of high school graduate (6/16, 38%) or higher (3/16, 19%), cardiac rehabilitation attendance or completion (3/16, 19%), no depressive symptoms (1/16, 6%) or anxiety (2/16, 13%), and high reported quality of life (1/16, 6%) or self-efficacy (1/16, 6%). Instruction of the peer supporters differed, but often included a variation of CHD educational resources and/or communication techniques that were delivered in training ranging from one to nine sessions (median 3, mode 1, and IQR 4) (Table 2).
Delivery, format, and content of peer support interventions
The most common delivery format was experience sharing (group discussion 5/16, 31%; individual 2/16, 13%), followed by presentations, role play, telephone conversations, clips/videos, brochures (2/16 each, 13%), and problem solving (1/16, 6%) (Table 2). Four studies (25%) did not report the format of the intervention. The content and topics that were delivered most frequently were medication management (8/16, 50%), managing psychological and emotional impacts (7/16, 44%), CHD and ACS mechanisms and causes (6/16, 38%), diet and nutrition (5/16, 31%), exercise (5/16, 31%), and self-management skills (5/16, 31%). Six interventions had content that was guided by the peer supporters (38%) whereas only one intervention (6%) was guided by the peers receiving the support. However, half of the studies (8/16, 50%) did not report how the intervention topics were guided or decided. Four studies (25%) cited Bandura’s self-efficacy theory as the underlying model behind the intervention.49
Effects of peer support interventions
Peer support interventions had no significant effect on the psychosocial outcomes of anxiety (7 studies: SMD −0.73, 95% CI −1.57, 0.10), depression (6 studies: SMD −0.09, 95% CI −0.25, 0.06), HRQoL (4 studies: SMD −0.38, 95% CI −1.84, 1.08), or perceived social support (2 studies: SMD −0.05, 95% CI −0.31, 0.21) (Figure 2). However, peer support improved self-management behaviours (4 studies; SMD 1.55, 95% CI 0.56, 2.54) and self-efficacy up to 6 months (5 studies: SMD 0.57, 95% CI 0.37, 0.77) and 6–12 months (2 studies, SMD 0.67, 95% CI 0.29, 1.05) (Figure 2). Peer support interventions significantly reduced the likelihood of hospital readmissions (3 studies; risk ratio 0.25, 95% CI 0.10, 0.60) (Figure 2). Statistical heterogeneity was substantial (I2 = ≥90%) for all outcomes apart from readmission, depression, and perceived social support (I2 = 0%). Subgroup analysis was not feasible for any of the outcomes due to high clinical heterogeneity between study characteristics. Sensitivity analysis confirmed the robustness of these findings, with individual exclusion of each study not changing the overall statistical significance or non-significance of the result of any of the pooled outcomes.
Narrative synthesis outcomes
Most studies reported improvements in one or more measured outcomes in the peer intervention study arms (see Supplementary material online, Material S3). Timing of peer support initiation may be influential, with interventions that were commenced during admission collectively demonstrating statistically significant improvements across almost all outcomes. Improvements were noted for anxiety,35,39,40,45,48 depression,45 HRQoL,35,42,45 self-management behaviours,35,37,40,42,44,45 self-efficacy,40,43,44 and readmission.43,45 The exception was for depression, which only improved in one study.47 In contrast, the majority of peer support interventions commenced post-discharge did not have a significant effect on the outcomes of anxiety,31,34,38,47 depression,31,38,47 perceived social support,34,38 self-efficacy,31,38,47 HRQoL,31,38,41,47 and self-management behaviours.31,47 Single studies only reported improvements HRQoL,46 self-management behaviours,46 and readmissions.34 Mode of delivery may be influential as well. With the exception of one study,31 all peer support studies delivered in person (either entirely or in combination) demonstrated an improvement in one or more outcome, including anxiety,36,39,40,48 HRQoL,35,41,46 self-management behaviours,35,37,40,46 self-efficacy,40,43 and readmissions43 (see Supplementary material online, Material S4). In contrast, telephone peer support interventions demonstrated no statistically significant effect on any outcome apart from readmissions34 and HRQoL41 in single studies. When a combination of different modes of delivery was used (i.e. in person, telephone, and messaging), improvements occurred across most outcomes,44,45 apart from in one study.47 Feasibility, acceptability, and cost-effectiveness were not investigated in any of the studies, although we did not specifically seek to explore these outcomes in the search strategy.
Risk of bias
The quality of the included studies was variable (Figure 3). Risk of bias was generally lowest for incomplete outcome data and selective outcome reporting but highest for sequence generation for randomization. The risk of bias was rated as ‘unknown’ for the majority of studies for allocation concealment and blinding, with these data commonly not reported. Only one study achieved low risk of bias across all appraisal domains.35 We were unable to conduct analysis of publication bias by using funnel plots, because generally at least 10 studies are recommended to distinguish chance from genuine asymmetry.33 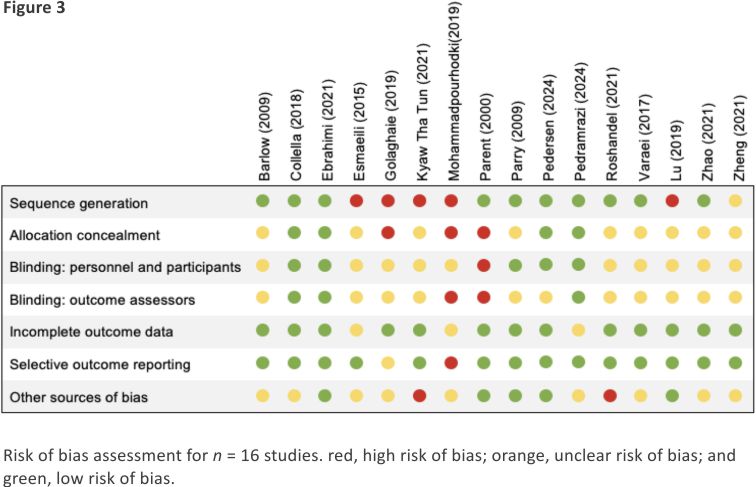
The findings of this systematic review and meta-analysis indicate that peer support interventions may be used to improve CHD self-management behaviours and self-efficacy and reduce readmission risk. However, meta-analysis revealed no significant differences in HRQoL, depression, anxiety, or perceived social support between those receiving peer support and those receiving usual care and heterogeneity prevented subgroup analysis from being undertaken. Narrative synthesis identified that most peer support interventions demonstrated improvements in at least one outcome compared with controls, and this was most consistently observed in peer support interventions that commenced during admission or that were entirely or partial in person. Anxiety, HRQoL, self-management behaviours, self-efficacy, and readmission were observed to improve in those receiving peer support across multiple studies. However, significant improvements in depressive symptoms were only observed in one study and peer support had no statistically significant effect on perceived social support. The most commonly used peer support strategies were in person, group-based, and experience sharing interventions. In interventions where content was determined, medication management, psychosocial impacts, diet, exercise, CHD mechanisms, and self-management were the most frequently discussed topics.
This review reveals that peer support interventions improved self-management behaviours at 6 months, improved self-efficacy up to a year, and reduced readmission risk after CHD diagnosis. This outcome is likely to be because higher self-efficacy and self-management behaviours are associated with higher adherence to secondary prevention, which is well established to lower readmissions in CHD.3 Self-efficacy and self-management have also been demonstrated to improve among people with cancer and Type 2 diabetes receiving peer support interventions.21,50 Although self-efficacy can independently improve after CHD diagnosis over time,51 these results suggest that peer support may enhance this process as pooled analysis indicated that self-efficacy was higher in those receiving peer support compared with usual care. This is because self-management often develops within a social context, contingent on community and external support.52 Self-management proficiency is also relative to an individual’s capacity for growth, including the ability to self-identify and address the perceived challenges one is experiencing.53 As such, self-efficacy and self-management are directly influenced by peer support, which foster confidence and the ability to cope, and are also indirectly influenced because peers provide camaraderie, decrease isolation, and provide a forum for problematic issues unable to be raised elsewhere. 54 Self-efficacy is also built when peers reciprocally support one another,54 and thereafter, the non-hierarchal nature of peer support enables participants to become their own advocate.18,55 As a result, learning occurs because peers simultaneously influence and are influenced by others in the environment in which the peer support is taking place.49 Moreover, interaction with peers provides vicarious experiences and verbal persuasion, which are key components of self-efficacy development.56
This review identifies that elements of CHD peer support interventions and the outcomes measures of each study are collectively diverse. While several studies did independently report improvements in anxiety and HRQoL in participants receiving peer support, there were no significant differences observed in the pooled analysis, consistent with systematic reviews of other conditions such as inflammatory bowel disease.57 A 2024 systematic review examining peer support interventions for patients with MI did not undertake meta-analysis but also concluded that peer support has a likely positive effect on depression, anxiety, and HRQoL, while acknowledging that heterogeneity was high.58 These findings suggest that the effectiveness of peer support on outcomes may vary in relation to how the intervention itself differs and the context it is delivered in. For example, peer support interventions that were delivered in person (entirely or in combination) demonstrated statisti-cally significant improvements across most outcomes, but most interventions delivered by telephone or commenced post-discharge did not. Although it was not possible to use subgroup analysis to investigate these results, similar findings have been identified in the wider literature, with subgroup analysis in both cancer and Type 2 diabetes peer support interventions demonstrating improvements in psychosocial outcomes that were not present in the overall meta-analysis.21,59
Although this review has identified 16 RCTs examining the effectiveness of CHD peer support, several gaps remain in the literature that this study emphasizes. Firstly, this review identifies that the individual peer support components are not always reported and seldom investigated within studies, a pervasive problem in the peer support literature,19 and future studies need to clearly identify and consider these elements in the analysis of results. Individual elements of peer support require further investigation to determine the relative influence on psychosocial, behavioural, and readmission outcomes among people with CHD. Another important consideration is the potential diversity in usual care varying between countries and the influence of the culture and context of each study, 60 including whether participants attended cardiac rehabilitation or not. Cardiac rehabilitation, for example, typically fosters natural peer support, which attenders report results in new behavioural changes, reduced alienation, a sense of normality, and a source of moral support,61 whereas cardiac arrest survivors report feeling understood for the first time.62 Although not within the aims of this review, it is also interesting to note that none of the included studies explored the feasibility, acceptability, or cost-effectiveness of peer support interventions, and no interventions included in this review were delivered online or via mobile application. It is important for peer support intervention developers to consider the preferences of the peer support attendees, including access, referral and participation, length of sessions, training of peer leaders, and timing of interventions to coincide with readiness for peer support participation.63
Strengths and limitations
To our knowledge, this is the first systematic review and meta-analysis specifically examining the impact of peer support interventions among people with CHD on psychosocial outcomes, self-care behaviours, and readmissions. However, limitations should be considered. Most outcomes were self-reported and measured with various instruments at different time points, leading to high statistical heterogeneity. Peer support interventions varied and several studies did not report all characteristics, which may limit generalizability and indicate that clinical heterogeneity may also be high. Although a high-sensitivity search strategy was developed in consultation with an academic liaison librarian, it is possible that some studies may not have been identified due to the diverse nature of peer support interventions. The control arm was not reported in two studies and was ‘usual care’ in others, which may differ by country. Additionally, the control arm of two studies included attendance at a cardiac rehabilitation programme, which in itself can expose participants to peer interaction (and thus natural peer support). Due to the limited number of studies, we were unable to assess publication bias using funnel plots, and it was not possible to explore the likelihood of negative results being withheld from publication, which could have influenced the generalizability of these findings.64 Subgroup analysis was not possible, and some analyses may have been underpowered. Future studies should investigate the effects of specific delivery formats and timeframes in various contexts, with repeated meta-analysis considered after additional RCTs on these outcomes.
Conclusion
Peer support interventions may be used to improve self-management behaviours and self-efficacy and reduce readmission for people with CHD. However, no statistically significant effect of peer support on anxiety, depression, HRQoL, or perceived social support was observed in the meta-analysis. Peer support interventions for CHD varied widely; however, most were delivered in face-to-face group-based experience sharing settings, whereas none were delivered in an online digital format. Although a number of RCTs investigating CHD peer support interventions were identified, specific components of the peer interventions were diverse, not always reported, and not able to be individually investigated. Further studies are needed with careful consideration of specific content, delivery, and contexts.
Acknowledgements
We thank Ms Judith Fethney for her time and expertise in checking the statistical methodology and Dr Karice Hyun for her statistical advice.
Author contributions
J.W. and R.G. contributed to conceptualization of this manuscript. J.W. and W.S. conducted investigation, data curation, and formal analysis including searching, screening, data extraction, and risk of bias assessment. R.G. provided consensus for disagreement resolution for screening and risk of bias. J.W. conducted meta-analysis and narrative synthesis and wrote the original draft and all subsequent versions. R.G., J.R., and T.B. provided doctoral supervision for J.W. All authors reviewed and edited the complete draft of the manuscript.
Funding
J.W. is funded by the SOLVE-CHD NHMRC Synergy Grant (GNT11 82301). J.R. is funded by a NHMRC Investigator Grant (GNT2007946). The funders had no role in the design and conduct of the study.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article and its Supplementary material.
References
1. Vaduganathan M, Mensah GA, Turco JV, Fuster V, Roth GA. The global burden of cardiovascular diseases and risk. J Am Coll Cardiol 2022; 80:2361 –2371.
2. de Oliveira LMSM, Costa IdC, da Silva DG, Silva JRSS, Barreto-Filho JAS, Almeida-Santos MA, et al. Readmission of patients with acute coronary syndrome and determinants. Arq Bras Cardiol 2019;113:42–49.
3. Rashidi A, Whitehead L, Glass C. Factors affecting hospital readmission rates following an acute coronary syndrome: a systematic review. J Clin Nurs 2022;31:2377–2397.
4. Astin F, Horrocks J, Closs SJ. Managing lifestyle change to reduce coronary risk: a synthesis of qualitative research on peoples’ experiences. BMC Cardiovasc Disord 2014;14:96.
5. Murphy B, Le Grande M, Alvarenga M, Worcester M, Jackson A. Anxiety and depression after a cardiac event: prevalence and predictors. Front Psychol 2019; 10:3010.
6. Jackson AC, Rogerson MC, Amerena J, Smith J, Hoover V, Alvarenga ME, et al. Unraveling the complexity of cardiac distress: a study of prevalence and severity. Front Psychiatry 2022; 13: 8089 04.
7. Sajobi TT, Wang M, Awosoga O, Santana M, Southern D, Liang Z, et al. Trajectories of health-related quality of life in coronary artery disease. Circulation 2018;11:e 003661.
8. Tod A. Exploring the meaning of recovery following myocardial infarction. Nurs Stand 2008;23: 35 –42.
9. Ski CF, Jelinek M, Jackson AC, Murphy BM, Thompson DR. Psychosocial interventions for patients with coronary heart disease and depression: a systematic review and meta-analysis. Eur J Cardiovasc Nurs 2016; 15:305–316.
10. Buursma MP, Tintle NL, Boven E, DeVon HA, Dunn SL. Lack of perceived social support in patients with ischemic heart disease is associated with hopelessness. Arch Psychiatr Nurs 2020; 34:14–16.
11. Zhou Y, Huo Q, Du S, Shi X, Shi Q, Cui S, et al. Social support and self-efficacy as mediating factors affecting the association between depression and medication adherence in older patients with coronary heart disease: a multiple mediator model with a cross-sectional study. Patient Prefer Adherence 2022; 16:285 –295.
12. Richards SH, Anderson L, Jenkinson CE, Whalley B, Rees K, Davies P, et al. Psychological interventions for coronary heart disease. Cochrane Database Syst Rev 2017;2017: Cd00 2902.
13. Sin NL, Kumar AD, Gehi AK, Whooley MA. Direction of association between depressive symptoms and lifestyle behaviors in patients with coronary heart disease: the heart and soul study. Ann Behav Med Publ Soc Behav Med 2016; 50:523–532.
14. Tovar E, Rayens MK, Gokun Y, Clark M. Mediators of adherence among adults with comorbid diabetes and depression: the role of self-efficacy and social support. J Health Psychol 2015;20:1405 –1415.
15. Redfern J, Hyun K, Chew DP, Astley C, Chow C, Aliprandi-Costa B, et al. Prescription of secondary prevention medications, lifestyle advice, and referral to rehabilitation among acute coronary syndrome inpatients: results from a large prospective audit in Australia and New Zealand. Heart 2014;100:1281– 1288.
16. Dolansky MA, Stepanczuk B, Charvat JM, Moore SM. Women’s and men’s exercise adherence after a cardiac event. Res Gerontol Nurs 2010;3:30– 38.
17. Bjarnason-Wehrens B, McGee H, Zwisler A-D, Piepoli MF, Benzer W, Schmid J-P, et al. Cardiac rehabilitation in Europe: results from the European Cardiac Rehabilitation Inventory Survey. Eur J Cardiovasc Prev Rehabil 2010;17: 410–418.
18. Hu J, Wang X, Guo S, Chen F, Wu Y, Ji F, et al. Peer support interventions for breast cancer patients: a systematic review. Breast Cancer Res Treat 2019; 174:325–341.
19. Thompson DM, Booth L, Moore D, Mathers J. Peer support for people with cronic conditions: a systematic review of reviews. BMC Health Serv Res 2022;22:427.
20. Agency for Clinical Innovation. Peer support; consumer enablement guide. https://aci.health.nsw. gov.au/projects/consumer-enablement/how-to-support/peer-support.
21. Zhang S, Li J, Hu X. Peer support interventions on quality of life, depression, anxiety, and self-efficacy among patients with cancer: a systematic review and meta-analysis. Patient Educ Couns 2022;105:3213 –3224.
22. Pedersen M, Stoier L, Egerod I, Overgaard D. Mastery of everyday life and social support needs in older vulnerable women with myocardial infarction and their relatives: a qualitative study. Eur J Cardiovasc Nurs 2021;20: 641–647.
23. Ryan RM, Deci EL, eds. Self-Determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness. New York: Guilford Press; 2017.
24. Hildingh C, Fridlund B. A 3-year follow-up of participation in peer support groups after a cardiac event. Eur J Cardiovasc Nurs 2004; 3:315 –320.
25. Isaksen AS, Gjengedal E. Significance of fellow patients for patients with myocardial infarction. Scand J Caring Sci 2006;20: 403– 411.
26. Parry M, Watt-Watson J. Peer support intervention trials for individuals with heart disease: a systematic review. Eur J Cardiovasc Nurs 2010;9:57–67.
27. Purcell C, Smillie S, Boon MH, Simpson SA, Taylor RS. Effectiveness of social network interventions to support cardiac rehabilitation and secondary prevention in the management of people with heart disease. Cochrane Database Syst Rev 2020;2021:CD01 3820.
28. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n 71.
29. McKenzie JE, Brennan SE, Ryan RE, Thomson HJ, Johnston RV, Thomas J. Defining the criteria for including studies and how they will be grouped for the synthesis. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al., eds. Cochrane Handbook for Systematic Reviews of Interventions. Chichester, UK: John Wiley & Sons, Ltd. p33–65.
30. Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. www. covidence.org.
31. Barlow JH, Turner AP, Gilchrist M. A randomised controlled trial of lay-led self-management for myocardial infarction patients who have completed cardiac rehabilitation. Eur J Cardiovasc Nurs 2009;8:293–301.
32. Higgins JP, Savovic J, Page MJ, Elbers RG, Sterne JA. Assessing risk of bias in a randomized trial. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al., eds. Cochrane Handbook for Systematic Reviews of Interventions. Chichester, UK: John Wiley & Sons, Ltd. p205–228.
33. Deeks JJ, Higgins JP, Altman DG, Group on behalf of the CSM. Analysing data and undertaking meta-analyses. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al., eds. Cochrane Handbook for Systematic Reviews of Interventions. Chichester, UK: John Wiley & Sons, Ltd. p241–284.
34. Colella TJF, King-Shier K. The effect of a peer support intervention on early recovery outcomes in men recovering from coronary bypass surgery: a randomized controlled trial. Eur J Cardiovasc Nurs 2018; 17:408– 417.
35. Ebrahimi H, Abbasi A, Bagheri H, Basirinezhad MH, Shakeri S, Mohammadpourhodki R. The role of peer support education model on the quality of life and self-care behaviors of patients with myocardial infarction. Patient Educ Couns 2021; 104:130– 135.
36. Esmaeili R, Jannati Y, Ghafari R, Charati JY, Jelodar HN. A clinical trial comparing the effect of peer education and orientation program on the anxiety levels of pre-CABG surgery patients. J Med Life 2015; 1:66–71.
37. Golaghaie F, Esmaeili-Kalantari S, Sarzaeem M, Rafiei F. Adherence to lifestyle changes after coronary artery bypass graft: outcome of preoperative peer education. Patient EducCouns 2019;102:2231–223 7.
38. Kyaw Tha Tun E, Nagel J, Bosbach A, Bock S, Kielblock B, Siegmund-Schultze E, et al. Telephone-based peer support intervention to reduce depressive symptoms in women with coronary heart disease, a randomized controlled trial in Germany. Women Health 2021; 61:619–632.
39. Mohammadpourhodki R, Bagheri H, Basirinezhad MH, Ramzani H, Keramati M. Evaluating the effect of lifestyle education based on peer model on anxiety in patients with acute myocardial infarction: randomized controlled trial of a peer based intervention on anxiety in patients with myocardial infarction. J Complement Integr Med 2019;16:/j/jcim. 2019. 16.issue-3/jcim-2018-0132/jcim-2018-0132.xml.
40. Parent N, Fortin F.A randomized, controlled trial of vicarious experience through peer support for male first-time cardiac surgery patients: impact on anxiety, self-efficacy expectation, and self-reported activity. Heart Lung 2000;29: 389–400.
41. Parry MJ, Watt-Watson J, Hodnett E, Tranmer J, Dennis C-L, Brooks D. Cardiac Home Education and Support Trial (CHEST): a pilot study. Can J Cardiol 2009; 25:e393– e3 98.
42. Roshandel M, Rakhshan M, Najafi Kalyani M. The effect of using peer on self-care, quality of life, and adherence in elderly people with coronary artery disease. Sci World J 2021;2021:47707 21
43. Varaei S, Shamsizadeh M, Cheraghi MA, Talebi M, Dehghani A, Abbasi A. Effects of a peer education on cardiac self-efficacy and readmissions in patients undergoing coronary artery bypass graft surgery: a randomized-controlled trial. Nurs Crit Care 2017; 22:19– 28.
44. Zhao K, Wang J. Application of peer education in cardiac rehabilitation of patients with coronary heart disease. ChinEvid-Based Nurs 2021;7: 2049– 2053.
45. Zheng F, Qiao L, Zhong Z, Duan Y, Ding S. Application of peer support intervention in the post-PCI nursing care of patients with acute myocardial infarction. Chin Nurs Res 2021;35:3581 –3587.
46. Lu H, Zhang J. Application of peer support education in continuing care of patients with coronary heart disease after PCI. Nurs Integr Tradit Chin West Med 2019;5: 144–147.
47. Pedersen M, Overgaard D, Boateng T, Bennich B, Beck AM, Andersen I, et al. The effect of peer-mentor support for older vulnerable patients with ischemic heart disease—a 24-week randomized controlled trial. J Cardiovasc Nurs 2024;DOI: 10.1097/JCN.00000 00000001158
48. Pedramrazi S, Mohammadabadi A, Rooddehghan Z, Haghani S. Effectiveness of peer-based and conventional video education in reducing perioperative depression and anxiety among coronary artery bypass grafting patients: a randomized controlled trial. J Perianesthesia Nurs 2024;39: 741–749.
49. Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. Englewood Cliffs, NJ: Prentice-Hall, Inc; 1986.
50. Chen C, Zhou Y, Xu J-Y, Song H-Y, Yin X-W, Gu Z-J. Effect of peer support interventions in patients with Type 2 diabetes: a systematic review. Patient Educ Couns 2024; 122:108172.
51. Kärner Köhler A, Tingström P, Jaarsma T, Nilsson S. Patient empowerment and general self-efficacy in patients with coronary heart disease: a cross-sectional study. BMC Fam Pract 2018; 19:76.
52. Grady PA, Gough LL. Self-management: a comprehensive approach to management of chronic conditions. Am J Public Health 2014;104:e2 5–e31.
53. Lorig KR, Holman H. Self-management education: history, definition, outcomes, and mechanisms. Ann Behav Med Publ Soc Behav Med 2003;26:1–7.
54. Jackson AM, Gregory S, McKinstry B. Self-help groups for patients with coronary heart disease as a resource for rehabilitation and secondary prevention –what is the evidence? Heart Lung 2009;38: 192–200.
55. Weddell J, Rogerson MC, Gallagher R, Hesselson S, Iismaa SE, Graham RM, et al. Cognitive and physical fatigue: the experience and consequences of ‘brain fog’ after spontaneous coronary artery dissection (SCAD), a qualitative study. Eur J Cardiovasc Nurs 2024; 23: 855–862.
56. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev 1977;84: 191–215.
57. Adriano A, Thompson DM, McMullan C, Price M, Moore D, Booth L, et al. Peer support for carers and patients with inflammatory bowel disease: a systematic review. Syst Rev 2022; 11200.
58.Heydari A, Manzari ZS, Mohammadpourhodki R. Peer-support interventions and related outcomes in patients with myocardial infarction: a systematic review. Heliyon 2024;10: e25314.
59. Kong L-N, Hu P, Yang L, Cui D. The effectiveness of peer support on self-efficacy and quality of life in adults with Type 2 diabetes: a systematic review and meta-analysis. J Adv Nurs 2019;75:711 – 722.
60. McEvoy JW, Jennings C, Kotseva K, De Bacquer D, De Backer G, Erlund I, et al. Variation in secondary prevention of coronary heart disease: the INTERASPIRE study. Eur Heart J 2024; 45:4184–4196.
61. Singh SKD, Noor ABYA, Ahmedy F, Abdullah KL, Abidin IZ, Suhaimi AB, et al. Exploring social support for women coping with a cardiac rehabilitation programme after acute coronary syndrome: a systematic review of qualitative studies. J Rehabil Med 2022;54:jrm00295.
62. Wagner MK, Kikkenborg Berg S, Hassager C, Joshi VL, Stenbæk DS, Missel M. Feeling understood for the first time: experiences of participation in rehabilitation after out-of-hospital sudden cardiac arrest. Eur J Cardiovasc Nurs 2021;20: 767–774.
63. Clougher D, Ciria-Suarez L, Medina JC, Anastasiadou D, Racioppi A, Ochoa-Arnedo C. What works in peer support for breast cancer survivors: a qualitative systematic review and meta-ethnography. Appl Psychol Health Well Being 2024; 16:793–815.
64. Joober R, Schmitz N, Annable L, Boksa P. Publication bias: what are the challenges and can they be overcome? J Psychiatry Neurosci 2012;37:149– 152.
Author notes
Conflict of interest: none declared.
Credits: Joseph Weddell, Wendan Shi, Julie Redfern, Thomas Buckley, Robyn Gallagher, Effectiveness of coronary heart disease peer support interventions: a systematic review and meta-analysis, European Journal of Preventive Cardiology, 2025;, zwaf241, https:// doi.org/10.1093 /eurjpc/zwaf241