

Jingjing Gao, 1 Yuyang Zhang, 1 Hu Li,1 Pan Gao, 1 and Xiansheng Zhang 1
Correspondence: should be addressed to Xiansheng Zhang; xiansheng-zhang@163.com
¹The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui Province, China
Academic Editor: Luisa Brussino
Abstract
It is an interesting clinical phenomenon that when evaluating the erectile function of men with erectile dysfunction by couples, respectively, using the erectile hardness model, there will exist the evaluation difference between men and their female partners. This phenomenon reflects the problem of communication and cognition between husband and wife in ED patients. To explore the influencing factors associated with this clinical phenomenon, we conducted this interesting, observational, and cross-sectional field survey. We enrolled 385 couples from the andrology clinics of the first affiliated hospital of Anhui Medical University from December 2017 to December 2018. The demographic data of couples, the medical history, sexuality and the characteristics of ED, and anxiety and depression of the couples were collected through face-to-face interview and questionnaires. The couples were divided into two groups containing 238 couples and 147 couples, respectively. We divided couples into difference group including couples which have inconsistent evaluation results from touching the erectile hardness model and no difference group including couples which have consistent evaluation results from touching the erectile hardness model, respectively. The difference group where the couples share different evaluation results reported higher erectile hardness grade from men than from their female partners (male > female: 73.11% vs. male < female: 26.89%). The scores of IIEF-5 in a different group and no difference group are 13.43 ± 5.75 and 16.82 ± 8.23, respectively. The average grades evaluated by men and women in the different group are 2.79 ± 0.85 and 2.45 ± 0.63, respectively. The average grades evaluated from couples in no difference group are 3.02 ± 0.45. Through statistical comparison and logistic regression analysis, duration of ED > 16 months, seeking treatment from female, negative communication state, and depression from men are the relevant factors accounting for the different evaluation results. This phenomenon reflects the problem of communication and cognition between husband and wife in ED patients. As for couples with these risk factors, we cannot focus only on the oral medication which only restores the penile erectile function. More importantly, we must combine sexual counselling and sexual knowledge education with drug treatment. When the two treatments are tightly integrated, not only the penile erection but also the gap of couples can be restored which is the best result of the ED treatment.
1. Introduction
Erectile dysfunction (ED), defined as the persistent inability to attain and/ or maintain an erection sufficient for sexual performance for at least six months, is one of the most common diseases in males 1. ED is a complicated interaction between the aetiology of vascular, neurogenic, hormonal, psychogenic, iatrogenic, and anatomic causes, which plays an important role in the occurrence of ED 2.
Several large epidemiological studies have shown a high prevalence and incidence of ED worldwide. In the Men’s Attitude to Life Events and Sexuality Study, which included 20 to 75-year-old men from 8 countries (United States, United Kingdom, Germany, France, Italy, Spain, Mexico, and Brazil), the ED prevalence, assessed by International Index of Erectile Function (IIEF), ranged from 22% in the United States to 10% in Spain 3. In a study surveying the prevalence of ED among type 2 diabetic Chinese men, among subjects with ED, the most prevalent was mild ED (28.9%), followed by mild-to-moderate (27.9%), moderate (13.4%), and severe (9%) ED 4. A project launched for estimating the likely worldwide increase in the prevalence of ED in the next 25 years projected that ED will affect 322 million by 2025 5. It is evident that ED has become a measurable health disorder for men globally that requires medical and public health attention.
ED has biological, psychological, and social effects on the patients and their sexual partners 6. A study conducted in China concluded that the prevalence of anxiety and depression were 79.82% and 79.56% in Chinese ED patients and the prevalence and severities of anxiety and depression increased as the ED severity increased 7. The effects of ED on the partners are strikingly similar to the effects on the patient. When erectile dysfunction occurs in a man, his female partner will suspect her attractiveness and worry that he is potent with other people. These anxious thoughts influence their confidence and lead to anxiety and depression 6. In conclusion, ED can cause frustration, anxiety, and depression for couples, potentially resulting in separation and/or divorce with the progress of the illness. The vicious cycle of anxiety and erectile dysfunction encompasses the entire relationship between the patient and the partner. With the development of this vicious circle, the couples will decrease the frequency of intercourse, time together, and communication 8. In addition, the Female Experience of Men’s Attitudes to Life Events and Sexuality study showed that women engaged less frequently in sexual activity after their partner developed ED and that their sex life was less satisfactory when the ED of their partner was severe. Similar results had been reported by other authors 9. A research found that compared to the general population, the quality of life in people with ED was known to be decreased to on average 10% 10. It concluded that ED not only harms the health of men but also damages the harmonious relationship between couples.
The emergence of phosphodiesterase type 5 inhibitor in 1998 dramatically altered the treatment landscape for erectile dysfunction 11. This targeted treatment is convenient for patients and physicians. The clinical efficacy of nonselective treatment for ED can reach 60%–80% 12. On the contrary, high rates of treatment discontinuation were present in several studies, ranging from 14% to 57% 13–16. Higher PDE5 discontinuation rates were found in other studies, reaching 80.4% 17. It is clear that there is a significant disparity between efficacy and continuation rates. Exploring this “disparity phenomenon,” we hypothesized that sexual dysfunction typically involves both physiological and psychological aspects, and such medications, although they improve penile neurovascular response, do not address the complex psychological and relationship issues that often accompany a sexual problem. Without exploring the relational issues that result from ED, the treatment efficacy would be limited.
In our daily male outpatient work, we found an interesting phenomenon: when using the erectile hardness measurement model for evaluating and comparing the erectile function of the men in the past six months, the couple who came to the male outpatient for ED came to a different conclusion. More often, the women’s response to erectile hardness is more objective and real than the patient himself. This phenomenon reflects the problem of communication and cognition between husband and wife in ED patients. In the general male population, the prevalence of ED has increased to approximately 20%, but less than 30% of patients seek treatment 18. Due to factors such as Chinese traditional culture, cognitional differences of the patients and their spouses, most men often show sorrow and anxiety about the disease and misconceive this disease. This makes the male patients in the face of the doctor only emphasize the organic factors of their erectile dysfunction, avoiding the related effects of the disease on the sexual partner and both sides. This will cause the doctor to ignore the effect of the ED on the patient’s relationship, and the treatment to the patient’s erectile function is limited to the use of drugs. However, except in ideal circumstances when these psychosocial forces are not present, dispensing a tablet to reverse these powerful forces is not likely to succeed 19. Consequently, the exploration of the influencing factor of the aforementioned details will be helpful to the exploration of the psychological factors owing to the illness itself and to attach sexual counselling and sexual education to the drug therapy to improve the treatment efficacy of ED.
The purpose of this paper is to explore the factors influencing the differences in the evaluation of the penile hardness model between husband and wife. We explore relevant factors from multiple perspectives including duration of ED, duration of the relationship, frequency of sexual intercourse, the main reason for the treatment of ED, the state of communication, and the psychological burdens of the couples. Moreover, we want to inform andrologists that when treating ED patients with such risk factors, combined drug therapy, sexual counselling, and sex education will achieve better therapeutic goals.
2. Methods
2.1. Patient Selection
Patients who were referred to the Department of Andrology, the First Affiliated Hospital of Anhui Medical University (Hefei, China), for the erectile dysfunction from December 2017 to December 2018, were enrolled in this study. This study was reviewed and approved by the Anhui Medical University Research Subject Review Board. Informed consent was obtained from all patients before the study. To be enrolled in the study, all subjects had to meet the following criteria: (a) males and their female partner aged ≥18 years; (b) the couples comprehend and speak Chinese, and (c) males having ED for more than six months with a regular heterosexual relation (at least once per week). Exclusion criteria were as follows: take a medicine that could affect erectile function, the presence of a severe psychopathological disorder, and suffering from premature ejaculation (according to the ISSM definition of PE). Subjects’ medical and sexual histories were carefully evaluated by an experienced clinician.
2.2. Study Design
Before the official investigation begins, a presurvey was given to a small sample (n = 30) to modify the originally designed items to ensure that the questionnaire was comprehensive and easily understood owing to several subjective and sensitive personal questions included in the study. This survey was conducted with three steps. Firstly, a question was asked to men with ED (diagnosed with IIEF-5) and their female partner, such as “based on the previous six months, which one of the models was similar to you or your partner erectile hardness.” Then, they answered the question by the evaluation model of erectile hardness (see Figure 1).
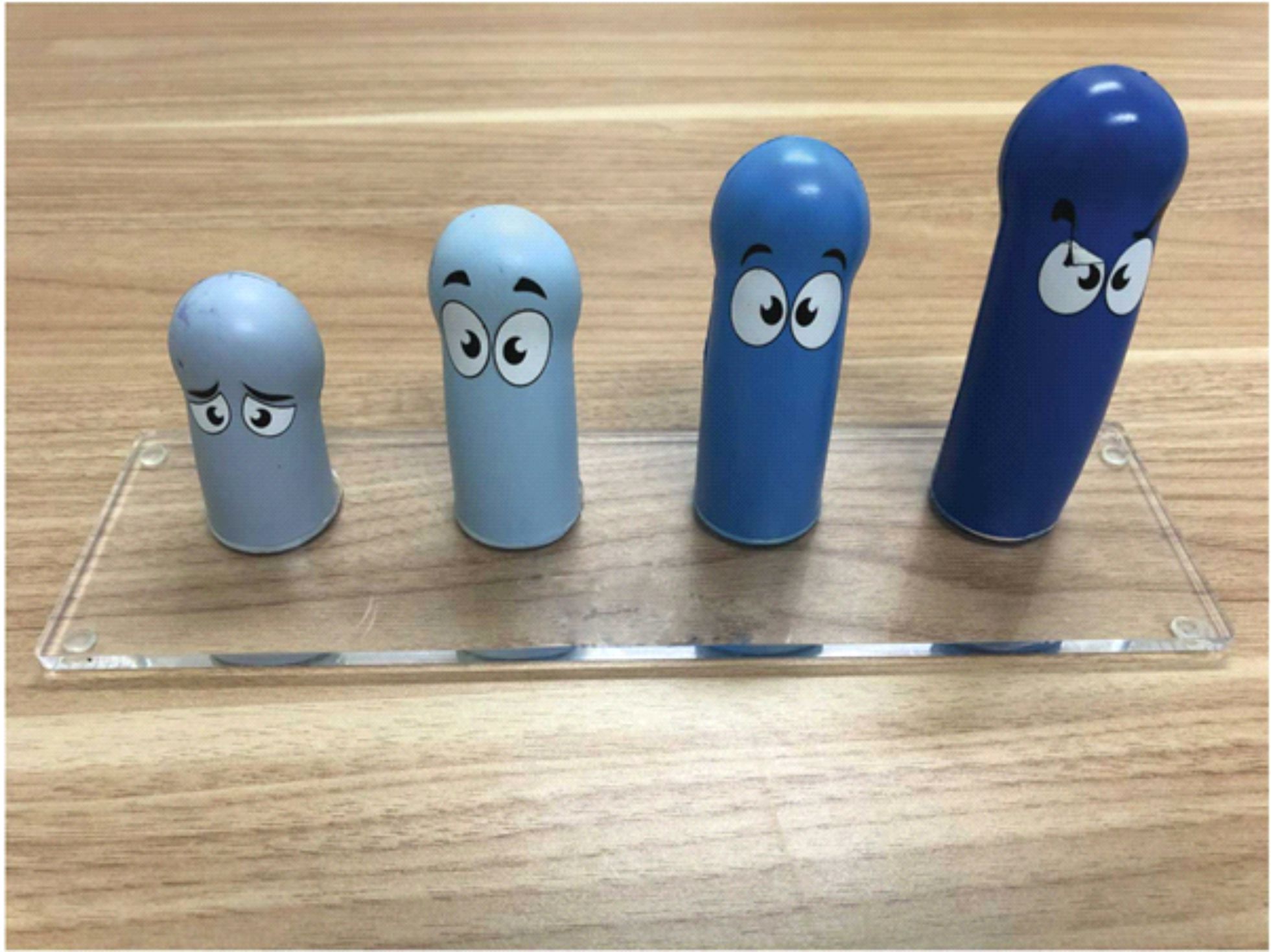
This model made by the Pfizer Inc. (Pfizer Inc., New York, NY) was the visual and tactile version of the standardized Erectile Hardness Score (EHS) tool 20. It was originally validated and standardized in order to evaluate the efficacy of sildenafil citrate in recovering EF 21. Its four grades represent four states of the penile, respectively when stimulated by the sex. The dark blue penis model of the tool (score 4 at the EHS) mirrors the sentence “penis completely hard and fully rigid.” The blue penis model of the tool (score 3 at the EHS), in turn, mirrors the sentence “penis hard enough for penetration but not completely hard.” The light blue penis model of the tool (score 2 at the EHS) mirrors the sentence “penis is hard but not hard for penetration.” The light grey penis model of the tool (score 1 at the EHS) mirrors the sentence “penis is large but not hard.” Secondly, a face to face interview was conducted to collect a detailed medical history of the patients, including the duration of the relationship, the cause of disease, the duration of disease, the frequency of sexual intercourse, the main reason of treatment, and the use of erectile-related drugs. Additionally, the state of couple communication includes active communication behaviour and negative communication behaviour 22. Thirdly, we make two questionnaires intended for men and women to collect some information. Here, a detailed interpretation of the questionnaires follows. The first part of the two questionnaires is the same, mainly including some demographic characteristics: age, BMI, lifestyle (smoking status and exercise status), characters, educational status, occupational status, and residence. The NEO-PI-R was used to assess the personality of the couples 23. The second part of the questionnaire intended for men is the 5 items of International Index for Erectile Function used to measure the sexual dysfunction of the men 24. The third part of the questionnaire attended for the couples contains the Zung self-rating anxiety/depression scales 25, 26. The reliability of these instruments (NEO-PI-R, the Zung self-rating anxiety/ depression scales, and IIEF-5) was assessed with Cronbach’s alpha coefficient. The internal consistencies of the NEO-PI-R, the Zung self-rating anxiety/depression scales, and IIEF-5 were 0.84, 0.80, 0.81, and 0.79, respectively.
According to NEO-PI-R, the personality was divided into introverts and extroverts 27, 28. Anxiety and depression, as the two indices reflecting the degree of negative psychological impact, were assessed by the Zung self-rating anxiety/ depression scales, in their Chinese version 29. Each questionnaire contained 20 questions. After the questionnaire was completed, the total scores for the Zung self-rating anxiety/depression scales were combined, divided by 80, and then compared with a standard cutoff score for anxiety or depression. A standard cutoff of 0.5 was employed such that a score <0.5 indicated no anxiety/ depression and a score _>0.5 confirmed anxiety/depression. The erectile dysfunction was measured by the Chinese version of IIEF-5 30, which is a validated five-item version of the 15-item IIEF questionnaire. It contains five questions, each of which is graded on a scale from 0 to 5 points. An IIEF-5 score >22 indicated normal erectile function and <22 indicated ED.
2.3. Main Outcome Measures
The main outcome was collected by combining a face-to-face interview with the questionnaires. First, demographic data of couples included age, BMI, lifestyle (smoking status and exercise status), characters, educational status, occupational status, and residence. Second, medical history and sexuality mainly contained the reason for treatment and the frequency of sexual intercourse. Third, the characteristics of ED included the duration of ED, the scores of IIEF-5, and the grades of EHS model evaluated by couples. Moreover, anxiety and depression of the couples were assessed by the Zung self-rating anxiety/depression scales, respectively.
2.4. Statistical Analysis
Data analyses were carried out with SPSS version 13.0 software (SPSS Inc., Chicago, IL, USA). Descriptive statistics were used to summarize the characteristics of the subjects. The descriptive data of subjects were expressed as the mean ± standard deviation or number (percentage) when appropriate. The independent t-test and chi-square test were used for intergroup comparisons. Multiple logistic regression analysis was used to evaluate the association between the factors of the couples and the different evaluation results of erectile hardness model. Odds ratios and 95% CIs were calculated to examine the strength of association. For all tests, value less than 0.05 was considered statistically significant.
3. Results
3.1. Characterization of the Two Groups
According to the evaluation results evaluated by couples through the erectile hardness model, we divided patients into different group and no difference group, respectively. The difference group (GROUP 1) included couples who have inconsistent evaluation results from touching the erectile hardness model. On the contrary, the no difference group (GROUP 2) included couples who have consistent evaluation results from touching the erectile hardness model.
3.2. Baseline Characteristics
Overall, a total of 385 couples are enrolled in our study. They all meet our inclusion criteria and are willing to participate in our research. According to the information completed by the study couples, two groups are generated. Of the total sample, 62% (238/385) of the sample were divided into the different group (GROUP 1) and 38% (147/385) of the sample were divided into no difference group (GROUP 2).
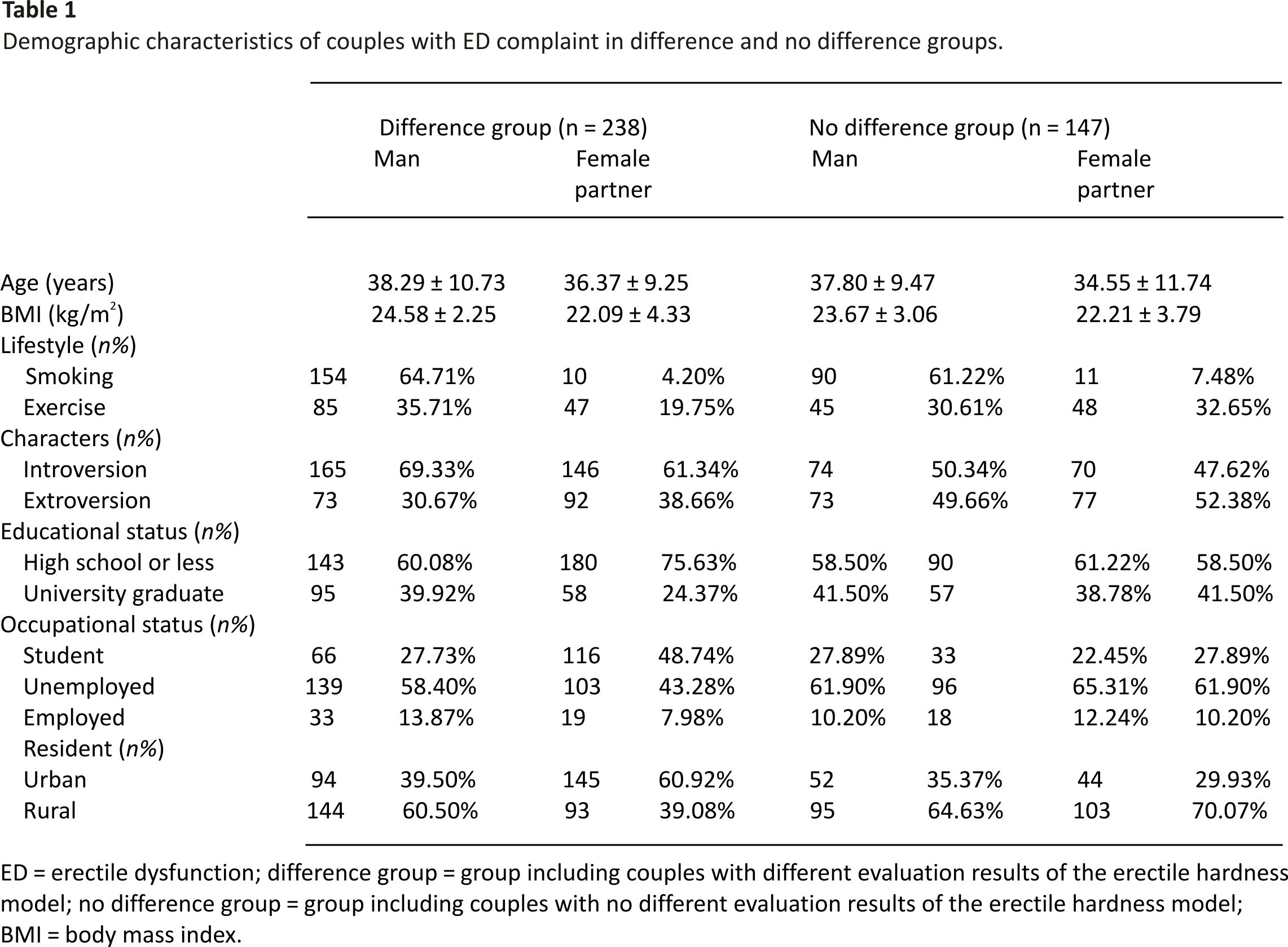
The demographic characteristics including age, BMI, lifestyle, characters, educational status, occupational status, and residence of the patients and the corresponding female partners are shown in Table 1. The t-test of two independent samples and the chi-square test were used for intergroup comparisons of the characteristics of the men and women, respectively. There was no statistical significance of the two groups no matter men or women.
3.3. Couples of the Difference Group
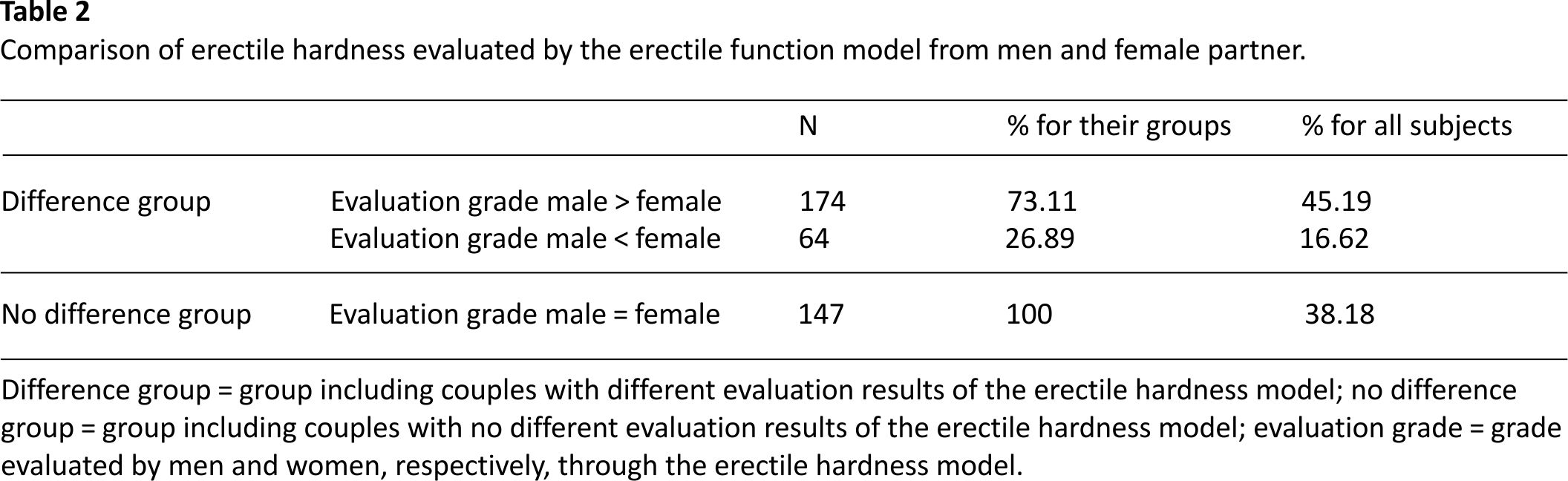
As shown in Table 2, the difference group not only consisted more couples but also report higher erectile hardness grade compared to the grade of their female partners (male > female: 147 (73.11%) vs. male < female: 64 (26.89 %)).
3.4. Factors Associated with Different Erectile Hardness Evaluation in Couples with ED
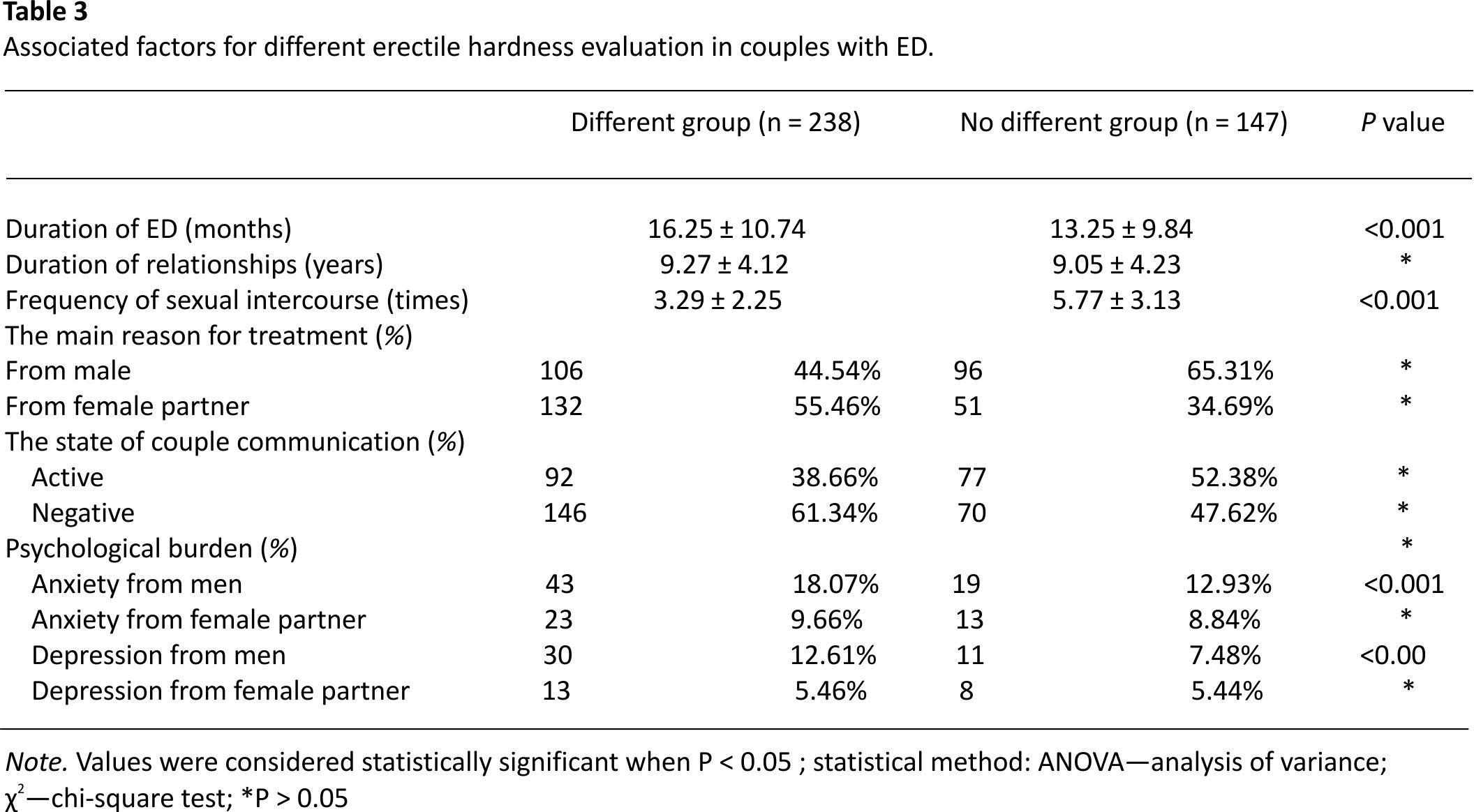
As shown in Table 3, we comparatively analyzed the couples’ sexual histories, the duration of ED, the frequency of sexual intercourse, communication state, and psychological burden. The significant differences were shown between difference group and no difference group with respect to duration of ED, frequency of sexual intercourse, the reasons of seeking treatment, the communication state of the couples, and several psychological burdens from men and women.
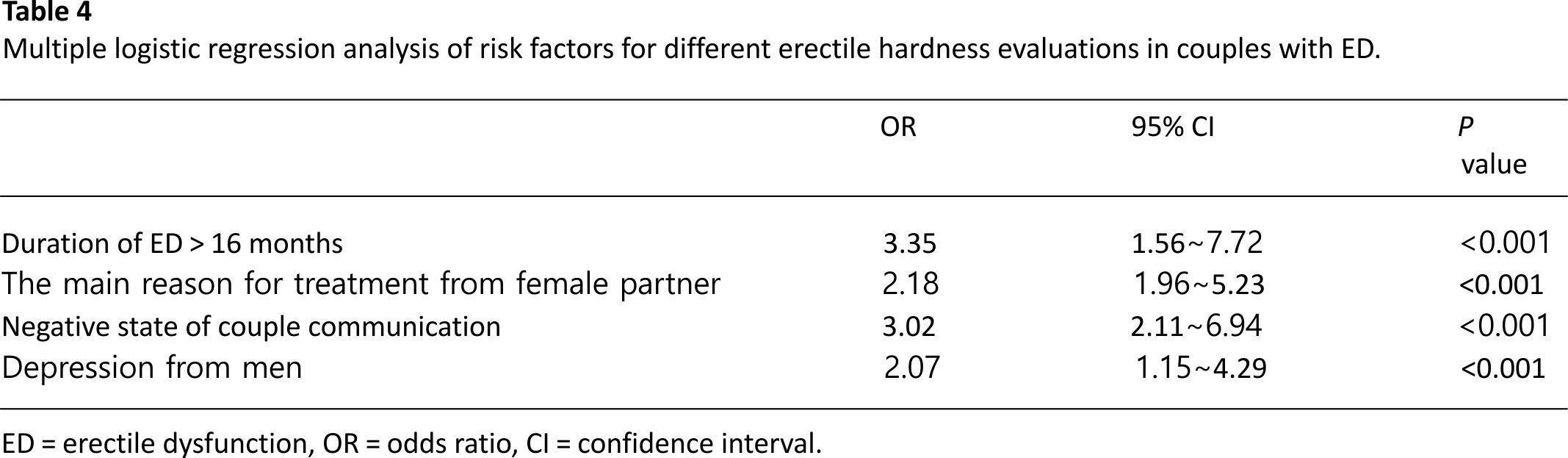
As shown in Table 4, logistic regression was conducted to assess whether the factors mentioned above could predict the evaluation difference. Through further correlation analysis, duration of ED > 16 months, seeking treatment from female, negative communication state, and depression from men were the factors associated with difference erectile hardness evaluation between couples.
3.5. Erectile Function of the Men in Two Groups
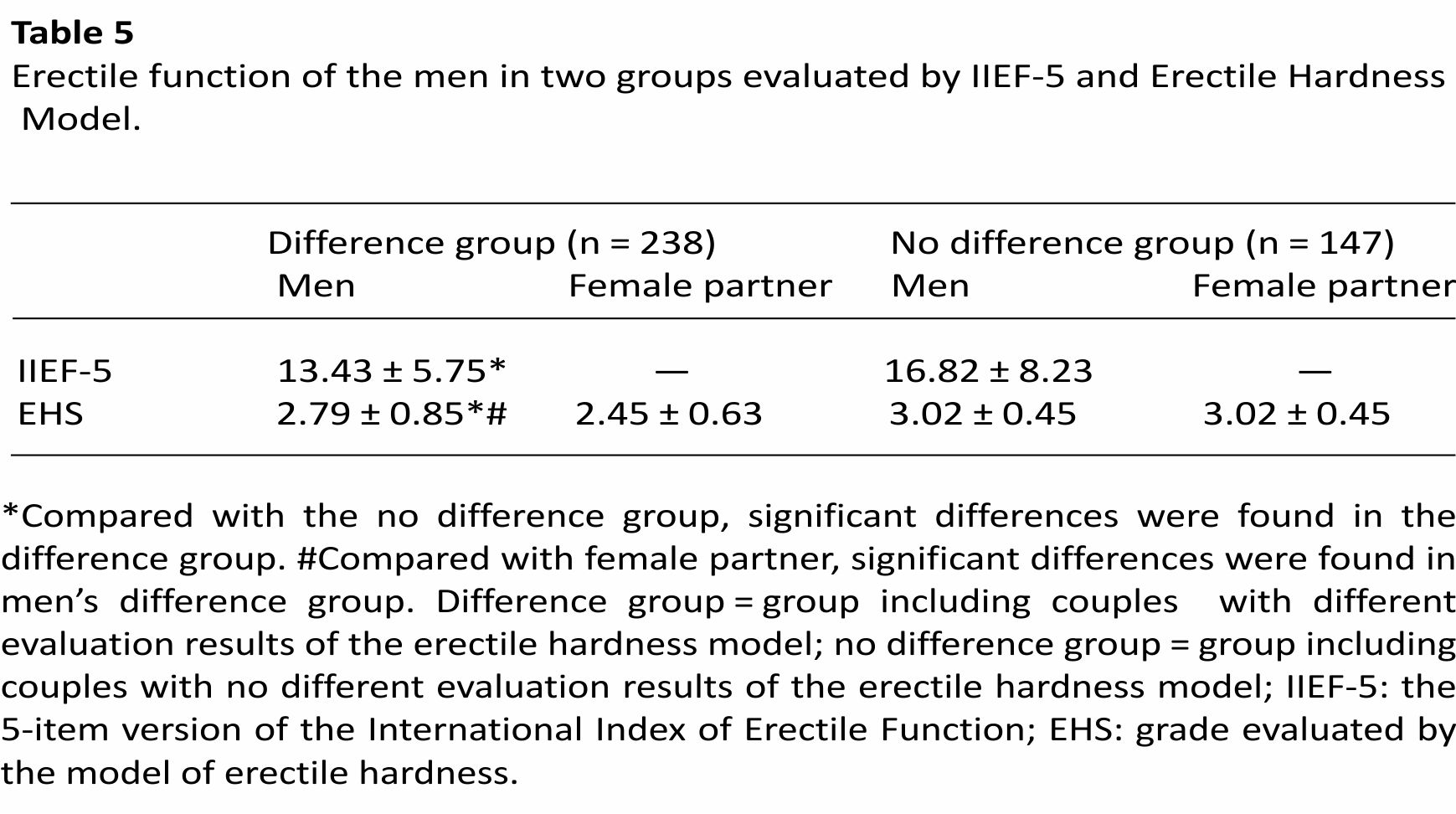
As shown in Table 5, the erectile function of the men was evaluated through the IIEF-5 by men and the erectile hardness model by the men and women. The scores of IIEF-5 in a different group and no difference group are 13.43 ± 5.75 and 16.82 ± 8.23, respectively. The average grades evaluated by men and women in the different group are 2.79 ± 0.85 and 2.45 ± 0.63, respectively. When compared with the no difference group, the men from difference group scored lower through IIEF-5. The results are the same as the method of the erectile hardness model. As mentioned above, the men from difference group scored lower through the erectile hardness model compared to their female partner.
4. Discussion
ED is a disease in which multiple factors are involved in the occurrence and the progression of it, and its aetiology is complicated 31. Among these factors, both husband and wife play an important role. In our clinical work, we find that as for men with erectile dysfunction, we need to not only evaluate the erectile function of the men and the related risk factors but also fully master how the relationship between husband and wife goes. Answers of these questions allow us to fully understand sexual cognition and the state of sexual communication of the two sides. When we treat men with ED only through drugs, we cannot restore these risk factors existing between couples which play important roles in the progress of the disease.
In our outpatient visit, we found that the husband and wife diverged on the evaluation of the male erectile function by the erectile function model when the couple visits us for ED together. The differences in sexual cognition and the lack of communication on sexual topics of couples were revealed through this simple phenomenon. This study was conducted to further explore the relevant factors affecting the evaluation results of couples. We concluded the factors that are closely related to the differences between the evaluation results of couples including the course of ED, the cause of treatment of ED patients, the communication status of couples, and the depression of men.
In this study, male patients in the different group were reported a longer course of ED than the no difference group. ED has a physical, mental, and social impact on the quality of life of patients and their partners 6. We think that the communication barrier between couples is prolonged as the duration of ED. For men, ED patients often show anxiety and depressive symptoms related to sexual performance. For women, this mental stress cannot be ignored. Changes in male sexual behaviour can confuse his sexual partners and even make her generate some strange ideas, such as their spouse is losing interest with her 32. The mental impact of ED on both men and women will gradually increase as the disease progresses, which will gradually undermine the sexual communication between the husband and wife. For women, male with ED also has a series of adverse effects on her sexual functions including sexual desire disorder, sexual excitement, orgasm disorder, and pain in sexual intercourse. A cross-sectional study conducted in Taiwan showed that women with ED partners had lower scores in FSFI’s total score and field scores compared with women without ED partners 33. Women continue to reduce sexual contact with patients because of these bad effects. Studies have also shown that when male patients developed ED, they also reduce the sexual life frequency of sexual partner to avoid embarrassing situation 34. The decline in sexual frequency will get worse as the duration of ED prolongs. It will reduce the quality of sexual life of both parties, reduce communication between husband and wife, and undermine the harmonious relationship between husband and wife.
For men, they are more likely to refuse treatment than women for most ailments 35. In China, influenced by the traditional culture of conservative attitude towards sex, men are even more reluctant to admit their decline in sexual function when faced with sex-related issues such as ED. A clinical-based survey in China named Help-seeking behaviour for erectile dysfunction found that many patients were clinically diagnosed with ED and might not realize that they had erectile problems at first 36. For women, they are always able to feel small changes in sexual behaviour during sexual intercourse earlier than men. Facing the embarrassing question of ED, the husband and wife have adopted two very different attitudes. This very different attitude led to assess differences in the face of the evaluation model. This conclusion agrees with our findings. These different attitudes of couples in the face of sexual problems will affect the treatment of ED. This also reminds us that in the process of ED treatment, sexual knowledge education and consultation for couples which are lacking in different groups are of great significance.
Our research indicates that the state of communication between husband and wife affects the judgment on the penile hardness model. The ED problem is not only a male problem but also a problem for couples. Culture defines the role of men and women, how they relate to each other, their cultural group, and the community 37. During the diagnosis and treatment of ED, women play an important role in the provision of patient medical history and patient compliance. The women’s understanding comes from the good communication between husband and wife and the correct understanding of sexual knowledge. Therefore, when the two sides communicate negatively, it will result in great resistance to the diagnosis and treatment of ED. In a study on the cessation of ED treatment, 9.3% of men pointed out that the relationship between husband and wife is the main reason for stopping drug treatment 38. So, when there is negative communication between the couple, this will inevitably lead to errors in their knowledge of the disease. When facing the hardness evaluation model, this error will be magnified. The phenomenon also reminds us that when treating ED patients, in addition to the use of drugs, we must deal with the communication state of the couples.
Mental factors are closely related to ED. In the United States, mental problems or stress are important predictors of ED and the OR is 3.6 39. Anxiety and depression are both risk factors for ED and important neurological effects of ED on men. ED and depression are considered to be two-way effects, and the two conditions reinforce each other 40. An estimated 25% of men with depressive symptoms may suffer from ED 41,42. Gradually, psychological disorders grew as the ED duration progressed. Not only the incidences but also the severities of anxiety and depression significantly rose with the duration of ED. Depression can reduce libido and aggravate the disease of ED 43. In the meantime, unsatisfied sexual life can aggravate depression. When men are suffering from depression due to ED, their attitude toward ED is more evasive. The evasive attitude will be uncovered when faced with a penile erection model.
Our research inspiration is from a small phenomenon found in Andrology outpatient work: different results between couples in using models to assess male erectile hardness grade. This small difference seems to have nothing to do with the treatment of ED. In fact, through our research, we find that there are many deep problems hidden under this phenomenon. Through in-depth analysis, we summarize four factors that influence the outcome, the duration of the ED, the reasons for the visit, the state of communication between the spouses, and the mental factors. These related factors also suggest that ED destroys not only the male penile erection function but also the relationship between husband and wife. The drug only treats the erectile function of the male, and the better treatment is to restore the harmonious sexual life of the patient and his wife. In response to these factors, sexual counselling and sexual education and drug therapy can be combined to achieve better therapeutic results.
There are some limitations in our article. (a) We performed the correlation research on the questionnaires of erectile dysfunction (IIEF-5) and the EHS from men and women. (b) This study is a cross-sectional study. Later, we will conduct a cohort study to further follow up patients in different groups to compare the response and continuation to PDE5i. (c) At the same time, we also conduct further research on the sexual function of the female partners using the Female Sexual Function Index. (d) In the later stage, we will carry out relevant sexual knowledge education and sexual counselling and apply the research results to the treatment of clinical ED.
5. Conclusion
ED not only affects the male penile erectile function but also destroy the sexual relationship and communication on sexual topics between couples. In our study, duration of ED > 16 months, seeking treatment from females and negative communication state and negatively psychological burden (depression) from men were the pivotal factors for different judgment grades between the spouses. As for couples with these risk factors, we cannot focus only on the oral medication which only restores the penile erectile function. More importantly, we must combine sexual counselling and sexual knowledge education with drug treatment. When the two treatments are tightly integrated, not only the penile erection but also the gap of couples can be restored which is the best result of the ED treatment.
Data Availability
Datasets supporting the conclusions of this article are available and can be requested from the corresponding author.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Authors’ Contributions
Jingjing Gao, Yuyang Zhang, and Hu Li contributed equally to this work.
References
1. M. Miner, M. T. Rosenberg, and J. Barkin, “Erectile dysfunction in primary care: a focus on cardiometabolic risk evaluation and stratification for future cardiovascular events,” The Canadian Journal of Urology, vol. 21, no. 2, p. 25, 2014. View at: Google Scholar
2. K.-K. Chew, A. Bremner, B. Stuckey, C. Earle, and K. Jamrozik, “Is the relationship between cigarette smoking and male erectile dysfunction independent of cardiovascular disease? Findings from a population-based cross-sectional study,” The Journal of Sexual Medicine, vol. 6, no. 1, pp. 222–231, 2009. View at: Publisher Site | Google Scholar
3. R. C. Rosen, W. A. Fisher, I. Eardley, C. Niederberger, A. Nadel, and M. Sand, “The multinational men’s attitudes to life events and sexuality (MALES) study I. Prevalence of erectile dysfunction and related health concerns in the general population,” Current Medical Research and Opinion, vol. 20, no. 5, pp. 607–617, 2004. View at: Publisher Site | ‘Google Scholar
4. W. Lo, S. Fu, C. H. Wong, and E. Chen, “Prevalence, correlates, attitude and treatment-seeking of erectile dysfunction among type 2 diabetic Chinese men attending primary care outpatient clinics,” Asian Journal of Andrology, vol. 16, no. 5, pp. 755–760, 2014. View at Publisher Site | Google Scholar
5. I. A. Ayta, J. B. McKinlay, and R. J. Krane, “The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences,” BJU International, vol. 84, no. 1, pp. 50–56, 1999. View at: Google Scholar
6. H. Li, T. Gao, and R. Wang, “The role of the sexual partner in managing erectile dysfunction,” Nature Reviews Urology, vol. 13, no. 3, pp. 168–177, 2016. View at Publisher Site | Google Scholar
7. Y. Yang, Y. Song, Y. Lu, Y. Xu, L. Liu, and X. Liu, “Associations between erectile dysfunction and psychological disorders (depression and anxiety): a cross-sectional study in a Chinese population,” Andrologia, vol. 51, no. 10, 2019. View at: Publisher Site | Google Scholar
8. F. Hedon, “Anxiety and erectile dysfunction: a global approach to ED enhances results and quality of life,” International Journal of Impotence Research, vol. 15, no. S2, pp. S16–S19, 2003. View at: Publisher Site | Google Scholar
9. W. A. Fisher, R. C. Rosen, I. Eardley, M. Sand, and I. Goldstein, “Sexual experience of female partners of men with erectile dysfunction: the female experience of men’s attitudes to life events and sexuality (FEMALES) study,” The Journal of Sexual Medicine, vol. 2, no. 5, pp. 675–684, 2005. View at: Publisher Site | ‘Google Scholar
10. S. E. Althof, “Quality of life and erectile dysfunction,” Urology, vol. 59, no. 6, pp. 803–810, 2002. View at: Publisher Site | Google Scholar
11. J. Mulhall, “Sildenafil: a novel effective oral therapy for male erectile dysfunction,” British Journal of Urology, vol. 79, no. 79, pp. 663-664, 1997. View at: Google Scholar
12. E. Christiansen, Sildenafil Multicentre Study Group, W. R. Guirguis, D. Cox, and I. H. Osterloh, “Long-term efficacy and safety of oral Viagra (sildenafil citrate) in men with erectile dysfunction and the effect of randomised treatment withdrawal,” International Journal of Impotence Research, vol. 12, no. 3, pp. 177– 182, 2000. View at Publisher Site | Google Scholar
13. C. Ljunggren, H. Hedelin, K. Salomonsson, and P. Ströberg, “Giving patients with erectile dysfunction the opportunity to try all three available phosphodiesterase type 5 inhibitors contributes to better long-term treatment compliance,” The Journal of Sexual Medicine, vol. 5, no. 2, pp. 469– 475, 2008. View at Publisher Site | Google Scholar
14. T. Klotz, M. Mathers, R. Klotz, and F. Sommer, “Why do patients with erectile dysfunction abandon effective therapy with sildenafil (Viagra)?” International Journal of Impotence Research, vol. 17, no. 1, pp. 2–4, 2005. View at: Publisher Site | Google Scholar
15. H. Son, K. Park, S. W. Kim, and J. S. Paick, “Reasons for discontinuation of sildenafil citrate after successful restoration of erectile function,” Asian Journal of Andrology, vol. 6, no. 2, pp. 117–120, 2004. View at: Google Scholar
16. B.-P. Jiann, C.-C. Yu, C.-C. Su, and J.-Y. Tsai, “Compliance of sildenafil treatment for erectile dysfunction and factors affecting it,” International Journal of Impotence Research, vol. 18, no. 2, pp. 146–149, 2006. View at: Publisher Site | Google Scholar
17. A. Salonia, A. Gallina, G. Zanni et al., “Acceptance of and discontinuation rate from erectile dysfunction oral treatment in patients following bilateral nerve-sparing radical prostatectomy,” European Urology, vol. 53, no. 3, pp. 564–570, 2007. View at: Publisher Site | Google Scholar
18. M. Kubin, G. Wagner, and A. R. Fugl-Meyer, “Epidemiology of erectile dysfunction,” International Journal of Impotence Research, vol. 15, no. 1, pp. 63–71, 2003. View at: Publisher Site | Google Scholar
19. S. E. Althof and M. Wieder, “Psychotherapy for erectile dysfunction: now more relevant than ever,” Endocrine, vol. 23, no. 2-3, pp. 131–134, 2004. View at: Publisher Site | Google Scholar
20. J. P. Mulhall, I. Goldstein, A. G. Bushmakin, J. C. Cappelleri, and K. Hvidsten, “Original research-outcomes assessment: validation of the erection hardness score,” The Journal of Sexual Medicine, vol. 4, no. 6, pp. 1626– 1634, 2007. View at Publisher Site | Google Scholar
21. I. Goldstein, T. F. Lue, H. Padma-Nathan, R. C. Rosen, W. D. Steers, and P. A. Wicker, “Oral sildenafil in the treatment of erectile dysfunction,” New England Journal of Medicine, vol. 338, no. 20, pp. 1397–1404, 1998. View at: Publisher Site | Google Scholar
22. H. C. Williams, X. Y. Ju, T. N. Bradbury, B. R. Karney, and X. Y. Fang, “Communication behaviour and relationship satisfaction among American and Chinese newlywed couples,” Journal of Family Psychology, vol. 26, no. 3, pp. 308–315, 2012. View at: Publisher Site | Google Scholar
23. P. T. Costa and R. R. McCrae, “Revised personality inventory (NEO PI-R) and NEO five-factor inventory (NEO-FFI),” Indian Streams Research Journal, vol. 2, 2012. View at: Google Scholar
24. R. Rosen, J. Cappelleri, M. Smith, J. Lipsky, and B. Peña, “Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction,” International Journal of Impotence Research, vol. 11, no. 6, pp. 319–326, 1999. View at: Publisher Site | Google Scholar
25. W. W. K. Zung, “A rating instrument for anxiety disorders,” Psychosomatics, vol. 12, no. 6, pp. 371–379, 1971. View at Publisher Site | Google Scholar
26. W. W. K. Zung, “A self-rating depression scale,” Archives of General Psychiatry, vol. 12, no. 1, pp. 63–70, 1965. View at Publisher Site | Google Scholar
27. H. J. Eysenck, “Genetic and environmental contributions to individual differences: the three major dimensions of personality,” Journal of Personality, vol. 58, no. 1, pp. 246–261, 1990. View at: Publisher Site | Google Scholar
28. X. I. Chang and M. T. Zhong, “Comparison of reliability and validity between full form and short form of big five personality scale neuroticism scale,” Chinese Journal of Clinical Psychology, vol. 25, no. 3, pp. 453–456, 2017, in Chinese. View at: Google Scholar
29. M. Y. Zhang, Manual of Psychiatric Rating Scale, Hunan Science and Technology Press, Changsha, China, 1993, in Chinese.
30. Y. F. Huang and H. J. Li, Practical Andrology, Science Press, Beijing, China, 2009, in Chinese.
31. G. M. Irwin, “Erectile dysfunction,” Primary Care: Clinics in Office Practice, vol. 46, pp. 249–255, 2019. View at: Google Scholar
32. F. A. Yafi, L. Jenkins, M. Albertsen et al., “Erectile dysfunction,” Nature Review Disease Primers, vol. 2, no. 1, pp. 1–20, 2016. View at: Publisher Site | Google Scholar
33. B. P. Jiann, C. C. Su, and J. Y. Tsai, “Is female sexual function related to the male partners’ erectile function?” The Journal of Sexual Medicine, vol. 10, no. 2, pp. 420– 429, 2013. View at: Publisher Site | ‘Google Scholar
34. R. Shabsigh, L. T. Klein, S. Seidman, S. A. Kaplan, B. J. Lehrhoff, and J. S. Ritter, “Increased incidence of depressive symptoms in men with erectile dysfunction,” Urology, vol. 52, no. 5, pp. 848–852, 1998. View at: Publisher Site | Google Scholar
35. P. M. Galdas, F. Cheater, and P. Marshall, “Men and health help-seeking behaviour: literature review,” Journal of Advanced Nursing, vol. 49, no. 6, pp. 616– 623, 2005. View at: Publisher Site | Google Scholar
36. K. Zhang, W. Yu, Z.-J. He, and J. Jin, “Help-seeking behaviour for erectile dysfunction: a clinic-based survey in China,” Asian Journal of Andrology, vol. 16, no. 1, pp. 131–135, 2014. View at: Publisher Site | Google Scholar
37. C. K. H. Christopher, P. Singam, G. E. Hong, and Z. M. Zainuddin, “Male sexual dysfunction in Asia,” Asian Journal of Andrology, vol. 13, no. 4, pp. 537–542, 2011. View at Google Scholar
38. A. A. Carvalheira, N. M. Pereira, J. Maroco, and V. Forjaz, “Dropout in the treatment of erectile dysfunction with PDE5: a study on predictors and a qualitative analysis of reasons for discontinuation,” The Journal of Sexual Medicine, vol. 9, no. 9, pp. 2361–2369, 2012. View at: Publisher Site | Google Scholar
39. E. O. Laumann, A. Paik, and R. C. Rosen, “Sexual dysfunction in the United States: prevalence and predictors,” The Journal of American Medical Association, vol. 281, no. 6, pp. 537–544, 1999. View at: Publisher Site | Google Scholar
40. A. B. Araujo, R. Durante, H. A. Feldman, I. Goldstein, and J. B. McKinlay, “The relationship between depressive symptoms and male erectile dysfunction: cross-sectional results from the Massachusetts male ageing study,” Psychosomatic Medicine, vol.
60, no. 4, pp. 458–465, 1998. View at: Publisher Site | Google Scholar
41. S. N. Seidman and S. P. Roose, “The relationship between depression and erectile dysfunction,” Current Psychiatry Reports, vol. 2, no. 3, pp. 201–205, 2000. View at: Publisher Site | Google Scholar
42. K. Williams and M. F. Reynolds, “Sexual dysfunction in major depression,” CNS Spectrums, vol. 11, no. S9, pp. 19–23, 2006. View at: Publisher Site | Google Scholar
43. A. W. Meisler and M. P. Carey, “Depressed affect and male sexual arousal,” Archives of Sexual Behavior, vol. 20, no. 6, pp. 541–554, 1991. View at: Publisher Site | Google Scholar
CREDITS: Jingjing Gao, Yuyang Zhang, Hu Li, Pan Gao, Xiansheng Zhang, “Different Evaluations Exist between Men with Erectile Dysfunction and Their Female Partners When Using Erectile Hardness Model: An Interesting, Observational, and Cross-Sectional Field Survey”, BioMed Research International, vol. 2020, Article ID 2302348, 8 pages, 2020. https://doi.org /10.1155/2020 /2302348






