

Kian Fan Chung1,2 and Stuart B. Mazzone3
1National Heart and Lung Institute, Imperial College London, London, United Kingdom; email: f.chung@imperial.ac.uk
2Department of Respiratory Medicine, Royal Brompton and Harefield Hospital, Guy’s and St. Thomas’ NHS Foundation Trust, London, United Kingdom
3Department of Anatomy and Physiology, University of Melbourne, Parkville, Victoria, Australia
ABSTRACT
Chronic cough can coexist with or without pulmonary and extra- pulmonary conditions and can be refractory to therapies that improve these associated conditions. It is underlined by cough hypersensitivity, which is characterized by increased cough responses to stimuli that affect the airways and vagally innervated tissues as well as by excessive cough responses to innocuous stimuli, and it is caused by neuroinflammatory and neuropathic mechanisms at both peripheral and central levels. The management of chronic cough starts with exclusion of associated conditions, followed by use of neuromodulators and speech and language therapy. This is progressing toward personalized management, with new approaches to endotype to treat these patients with the introduction of novel antitussive therapies.
Keywords
refractory chronic cough, unexplained chronic cough, cough hypersensitivity syndrome, laryngeal hypersensitivity, urge to cough, antitussives
FROM CHRONIC COUGH TO COUGH HYPERSENSITIVITY
Cough is a common complaint that doctors in primary and secondary care have to deal with, which is not surprising when chronic cough affects ∼10% of adults, with the prevalence being higher in Europe and America 1. The interest in chronic cough was ignited by the publication of an anatomical diagnostic protocol for its management by Irwin and colleagues in 19812, which emphasized excluding common conditions such as asthma, rhinosinusitis, and gastro-esophageal reflux that affect the structures within the anatomical distribution of the vagal afferent nerves.
This approach, which recognized that cough can be a defensive protective reflex mediated through the activation of cough receptors present in the upper and proximal intrapulmonary airways, became the cornerstone for managing chronic cough. The pathways regulating the cough reflex as a defensive mechanism had been described as involving various sensory receptors, known as cough receptors due to their conductive properties, with the afferent signals that they conduct carried via the vagus nerves to the nucleus tractus solitarius in the brainstem 3.
It was initially proposed that the cause of chronic cough can be determined 88–100% of the time, leading to successful treatment in 84–98% of patients 4. However, it became clear that there were chronic cough patients whose cough did not respond to treatment of any associated cause or who had no diagnosis or etiology associated with their cough5. This group, initially labeled as idiopathic chronic cough, ranged from 7% to 40% despite intensive investigations 5. With the definition of chronic cough being a cough that has lasted for more than 8 weeks, this subgroup of idiopathic cough came to be recognized as refractory chronic cough (RCC) or unexplained chronic cough (UCC) 6. Using patient-reported outcome tools to assess the impact of chronic cough, patients with chronic cough were found to have reduced quality of life, increased anxiety, exhaustion, and insomnia, which in turn impacted personal relationships, causing depression, self-isolation, and lower productivity at work 7, 8.
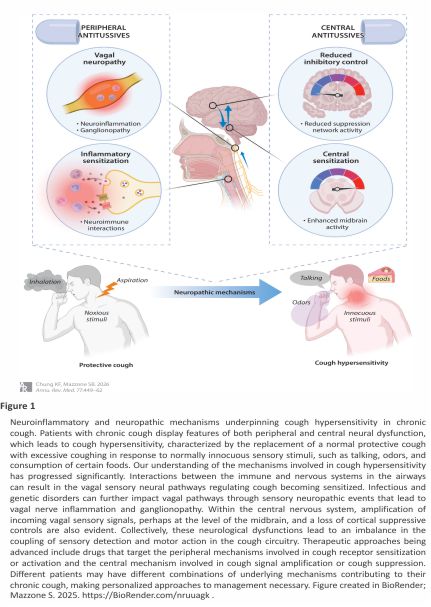
The concept of cough hypersensitivity underlying chronic cough was proposed in 2010 9,10 and changed the way clinicians and researchers picture the condition. Cough hypersensitivity syndrome has been defined as troublesome coughing often triggered by low levels of thermal, mechanical, or chemical exposure. The concept of an overwhelmed repetitive protective cough reflex was quickly replaced with that of a hyperresponsive behavior underscored by neuropathic processes and neural damage caused by a range of inflammatory, infective, and allergic factors impacting peripheral and central nervous system pathways 11 ( Figure 1 ).
 COUGH HYPERSENSITIVITY AS A NEUROPATHIC COUGH
COUGH HYPERSENSITIVITY AS A NEUROPATHIC COUGH
Peripheral Neural Mechanisms in Cough Hypersensitivity
Disordered neural function in chronic cough was initially presumed to occur at the level of the peripheral cough-evoking vagal sensory nerve fibers innervating the airways. Two types of vagal cough-evoking sensory nerve fibers exist (Aδ fibers and C fibers), enabling the detection of stimuli across broad physical, thermal, and chemical modalities 3. Cough may also be facilitated or inhibited by sensory inputs from other regions, including the nose, gut, ear, and skin, through convergent interactions with the central nervous system pathways involved in cough regulation 12. In preclinical animal studies, vagal cough-evoking sensory neurons become sensitized in response to prostaglandins, cytokines, bradykinin, adenosine triphosphate (ATP) and other classical inflammatory chemicals released by resident or recruited immunological cells, inhaled environmental chemicals, changes in air temperature, and molecules produced and released directly by pathogens 3. Furthermore, vagal sensory fibers may also be modulated by inhaled environmental chemicals, changes in air temperature, and even molecules produced and released directly by pathogens 13,14. When activated, vagal sensory neurons also contribute to the regulation of local airway inflammation via the release of neuroinflammatory peptides, such as substance P and calcitonin gene-related peptide 3 ( Figure 1 ).
It is not uncommon for chronic cough to occur in the absence of any identifiable airway pathology 6, which indicates that peripheral sensitization may not be a universal mechanism of cough hypersensitivity. Alternatively, the vagus nerve itself may develop an inflammatory response under some circumstances, contributing to altered vagal sensory function ( Figure 1 ). Persistent vagal neuroinflammation has been shown to be secondary to acute lung injury or infection, including in studies of lung fibrosis, influenza virus infection, and bacterial or allergen exposure 15. This neuroinflammation is associated with transcriptional, cellular, and structural vagal plasticity, which may contribute to hypersensitivity. Thus, airway biopsies from patients with chronic cough show signs of increased nerve fiber density and branching 16, which is expected in response to vagal neuroinflammation. Additionally, 10–20% of patients after COVID-19 infection and up to 43% of patients after H1N1 infection have persistent cough beyond the typical timeframe of infection pathogenesis 17,18, suggesting that the mechanisms responsible for persistent cough are unrelated to the presence of an ongoing infectious airway pathology. Anecdotally, it is also not uncommon for chronic cough to start after experiencing cold or flu symptoms many years prior.
Central Neural Mechanisms in Cough Hypersensitivity
Alterations in brain processing also play an important role in cough hypersensitivity and chronic cough 19, resembling processes that occur in nociplastic pain syndromes characterized by augmented central sensory processing and altered sensorimotor modulation 20 ( Figure 1 ). Vagal sensory fibers project to the brainstem, where inputs can reflexively regulate the respiratory neural circuits that generate breathing patterns 6. Ascending projections from the brainstem reach sensory, motor, prefrontal, and limbic cortices in the higher brain 19. The urge to cough is encoded at these higher brain levels, along with the accompanying affective (i.e., emotional) dimensions of coughing. Higher brain motor systems, in turn, provide a level of behavioral and cognitive control over cough, which can include pathways that both facilitate and inhibit coughing.
Longer chronic cough duration has been associated with a lower volume of brain gray matter in frontal lobe cortical regions 21, as well as with enhanced functional connectivity within the left frontoparietal cortical network associated with greater cough severity scores and a greater psychological and social impact of coughing 21. Functional imaging of the brain during experimentally induced urge to cough showed that patients with cough hypersensitivity have relatively normal lower brainstem processing responses (and therefore normal sensory nerve fiber inputs to the brainstem) during inhalation of cough stimuli, whereas higher brain circuit responses are increased 22, suggesting central amplification of cough signals. Thus, an amplifier of cough signals may exist in the brains of chronic cough patients, meaning that even low levels of sensory nerve activity are sufficient to evoke coughing. Patients also display reduced ability to volitionally suppress cough when challenged with an inhaled stimulus 23, unlike individuals without chronic cough, who can volitionally suppress evoked cough through the activation of motor suppression brain networks 19,24. Consequently, chronic cough could be considered a problem of increased central coupling of sensation to motor action, perhaps like that seen in patients with restless legs syndrome, where the urge-to-move sensation drives periodic limb movements 25. These changes in central cough processing may manifest as part of a central neuroinflammatory state orchestrated by brain glial cells 26. Interestingly, not all patients with chronic cough may have diminished central suppressive controls, as cough suppression appears to be unaffected in patients with chronic cough associated with chronic obstructive pulmonary disease 27. This observation further supports the existence of distinct cough endotypes28.
HETEROGENEITY OF COUGH HYPERSENSITIVITY–ASSOCIATED CONDITIONS
Clinical Aspects of Cough Hypersensitivity
Patients with chronic cough, particularly those with UCC or RCC, present with features of cough hypersensitivity and very often with features of laryngeal paresthesia, which is characterized by a persistent or intermittent tickling, irritating, or obstructive (i.e., globus) sensation in the pharynx or larynx 29. This is described by patients as itching or choking sensations in the throat that precipitate bouts of often severe coughing, either spontaneously or in response to mild or otherwise innocuous stimuli ( Figure 1 ). There is an accompanying perception of an urge to cough, analogous to the need to scratch an itch 30, which may not always be satiated by coughing, and this sensation can be more troubling to patients than the cough itself 29. Other symptoms common in patients with chronic cough include repeated clearing of the throat in attempt to clear the globus sensation or abate the urge to cough, chest tightness, dysphonia (i.e., hoarse voice), vocal cord dysfunction, and dysphagia, many of which are the result of laryngeal hypersensitivity 6, 31.
Refractory and Unexplained Chronic Cough
RCC and UCC patients are commonly recruited into clinical trials of new antitussives, if they score their cough severity as more than 40 mm on a 100 mm visual analog scale. In 2,044 such chronic cough patients, 75% were female, the mean age was 58 years, and 62% were diagnosed as RCC [with a diagnosis of asthma, gastroesophageal reflux disease (GERD), or upper airway cough syndrome (UACS)] and the rest as UCC; baseline cough characteristics were similar between RCC and UCC, with a mean duration of cough of 11.2 years and a cough frequency of 19.2/h 32. They had characteristics of cough hypersensitivity as determined by a high score on the Hull Airway Reflux Questionnaire.
Asthma and Eosinophilic Type 2 Inflammation
Asthma can present with cough as the sole or predominant symptom, with or without wheezing or dyspnea. Chronic cough in asthma has been associated with worse asthma severity and poorer outcomes, and cough worsening or onset has the highest prediction for progression to severe asthma 33,34. Cough reflex hypersensitivity to capsaicin has been associated with greater exacerbation rates and poorer asthma control 35 as well as with associated comorbidities in severe asthma 36. Capsaicin cough hypersensitivity has been demonstrated in adults with asthma 37, and laryngeal hypersensitivity is present in 87% of asthma patients presenting with laryngeal dysfunction 38. Type 2 inflammation characterized by eosinophilic airway inflammation may underlie cough hypersensitivity in asthma through the interaction of eosinophils with airway nerves that could lead to increased airway nerve densities 39. Products of activated eosinophils such as major basic protein can increase the sensitivity of C fibers to chemical and mechanical stimuli 40. Airflow obstruction may underlie the cough of asthma potentially through the release of mediators such as ATP that may sensitize sensory nerves or through the activation of mechanosensitive afferent airway nerves 41.
Upper Airway Cough Syndrome
UACS, previously known as postnasal drip or nasal catarrh, is caused by upper respiratory disorders, including rhinosinusitis 42. It is diagnosed based on a chronic cough associated with rhinitis or rhinosinusitis and its response to an H1 receptor antagonist and/or nasal anti-inflammatory corticosteroid therapy. Postnasal drip is the term preferred by Europeans, who consider it a symptom of cough caused by upper airway disease 43. The drip at the back of the nose can stimulate the afferent sensory nerves of the pharynx and larynx or even of the lower airways, although only 21% of subjects with postnasal drip report having chronic cough 44. Airway remodeling that may have been caused by the drip has been reported in UACS patients 45. Compared to healthy controls, increased cough sensitivity was noted in allergic rhinitis patients, a difference that became more prominent during the pollen season 46, with the release of histamine in the nasal space sensitizing the nasal sensory nerves to capsaicin 47.
Gastro-Esophageal Reflux Disease
GERD-associated cough is another common cause of chronic cough, accounting for 10–40% of chronic cough worldwide 48. It is often triggered or made worse by a meal and may occur with or without acid regurgitation or heartburn, which may be accompanied by hoarseness and throat clearing, induced by the direct effect of GERD or by the accompanying postnasal drip (i.e., laryngopharyngeal reflux). Abnormal acid or nonacid reflux can be detected by esophageal reflux monitoring of acid exposure time.
The direct effect of acid or nonacid reflux from the stomach in the proximal esophagus and larynx, that is, activating cough receptors, is likely a mechanism for chronic cough. In addition, airway reflux consisting of a gaseous mist of nonacid contents, diagnosed by pH-impedance measurement, has been proposed. Alternatively, an esophageal afferent nerve mediated esophagus-tracheobronchial reflex has been associated with increased sensitivity of the cough reflex following the development of neurogenic airway inflammation 49,50. In support of this, esophageal infusion of acid has led to increased cough sensitivity in patients with GERD and cough 51,52. Esophageal motility may increase the duration of esophageal acid exposure with slower clearance of acid, leading to more severe mucosal damage and more frequent reflux episodes 53. Finally, chronic cough can be an extraesophageal symptom of eosinophilic esophagitis, even without any gastrointestinal symptoms 54.
Interstitial Lung Disease
Interstitial lung disease (ILD) consists of pulmonary conditions characterized by inflammation and/or fibrosis of the lung parenchyma leading to progressive dyspnea and frequently to respiratory failure. Cough is present in 50–90% of patients with interstitial pulmonary fibrosis (IPF), a common form of ILD 55, and can be relentless, with one-third of patients indicating that cough is a worse symptom than dyspnea 56. Subjective quality of life scores and objective cough counts indicate a moderate to severe cough 57.
An increase in capsaicin and external percussion cough sensitivity in IPF has been reported 58,59. The cough hypersensitivity may be related to abnormal epithelial repair with the release of growth factors such as transforming growth factor beta and nerve growth factor 60. Mechanical distortion of the airways from fibrosis may lead to the activation of cough receptors, potentially mediated through TRPV4 receptors. Comorbid conditions such as GERD and UACS may also contribute 61.
Post-COVID Cough
Respiratory viral infections are typically accompanied by an acute cough that can persist for weeks or months in some patients. Cough reflex hypersensitivity to chemical and mechanical stimulation has been shown in experimental models of rhinovirus infections 62, 63. Studies of the recent COVID-19 pandemic have focused on the post-viral complications of long-COVID or post-COVID syndrome, including a wide array of symptoms, such as brain fog, tiredness, arthralgia, headaches, fever, skin rashes, and emotional disturbances 64. In the respiratory system, chest pain, breathlessness, and cough are common and may be associated with pulmonary dysfunction. The prevalence of post-COVID cough is reported to be ∼18% in patients who required hospitalization 17. Cough has been reported as the most common symptom, found in 92% of patients in the acute phase, with persistence of cough at 3 weeks or longer occurring in 13%, in whom the associated risk factors were diabetes, asthma, and chronic cough 65. Post-COVID persistent cough is similar in clinical characteristics to chronic cough, with a higher proportion of those with post-COVID cough expressing high levels of exhaled nitric oxide 64. The cough is characterized by both cough and laryngeal hypersensitivity 66. While the mechanisms responsible for persistent cough are unrelated to the presence of an ongoing infectious airway pathology, one mechanism may involve the direct invasion of SARS-CoV-2 into sensory nerves to alter sensory neuronal function mediating cough and to induce central sensitization 17.
Cerebellar Ataxia, Neuropathy, and Vestibular Areflexia Syndrome
Cerebellar ataxia, neuropathy, and vestibular areflexia syndrome (CANVAS) is a rare genetic disease caused by a multiple repeat expansion in the gene encoding replication factor complex subunit 1 (RFC1) 67. Patients with CANVAS develop progressive peripheral sensory neuropathy, ataxia, and balance disorder. The neuropathy is characterized by peripheral nerve atrophy and loss of sensory nerve action potentials on nerve conduction studies.
A persistent, irritating, dry, spasmodic cough is an early presenting symptom, preceding walking difficulties by several decades 68,69. Cough mainly occurs during the day and can be triggered by factors such as emotion, stress, speaking, or swallowing. It has a relentless clinical course with no seasonal fluctuations. Mechanical stimulation of the external ear canal innervated by the auricular branch of the vagus nerve triggers coughing via the Arnold nerve cough reflex, representing cough hypersensitivity along vagal sensory neural pathways 70.
In 6–25% of patients with RCC, there is at least one monoallelic repeat expansion in the RFC1 gene 71,72. The mechanisms leading to vagal hypersensitivity in CANVAS are unclear. Cough could occur with progressive neuronopathy, with a state of sensory hypersensitivity prior to sensory neuron destruction 73,74. In later stages, the denervation of brainstem neurons receiving sensory inputs may lead to spontaneous activity of central cough-evoking pathways with deafferentation hypersensitivity 75.
MANAGEMENT OF PATIENTS WITH CHRONIC COUGH HYPERSENSITIVITY
Excluding Treatable Causes of Chronic Cough
The first step in the evaluation of chronic cough is to exclude any underlying treatable cause using an anatomical diagnostic–therapeutic approach 76,77. For asthma, use of fractional exhaled nitric oxide and blood eosinophil count may be useful to predict the response to inhaled cortico-steroids and anti-leukotrienes. A course of oral corticosteroids may be needed. For UACS, a trial of an anti-H1 histamine antagonist, which may include a first-generation anti-H1 antagonist, or topical corticosteroids, both with trial of a course of antibiotics, may be needed. For GERD, reflux preventive measures and anti-reflux therapies should be tried in those with a history of heartburn. Investigations regarding nonacid reflux could be considered in case of lack of effect of anti-reflux medications.
Treatment of Chronic Cough and Cough Hypersensitivity
Centrally acting neuromodulators as antitussives.
Slow-release morphine can be partially effective in controlling severe chronic cough 78, although it is not universally recommended. Codeine, the methyl ether of morphine, was once common in cough syrups and previously the benchmark drug against which the efficacy of newer drugs was measured. Although codeine has little clinical efficacy in chronic cough, it is still used by some patients with variable effects 79. At their effective doses, opiates cause a range of undesirable side effects, including physical dependence, sedation, respiratory depression, and constipation.
Other centrally acting neuro- modulators, including gabapentin, pregabalin, baclofen, and amitriptyline, represent important treatment options for chronic cough 80, in line with their reported efficacy in neuropathic pain, because of their actions on the spinal and higher brain networks regulating pain processing 81. A systematic review of the clinical trial literature on gabapentin suggests that chronic cough patients commonly experience improvements in subjective cough severity and quality of life 80. Gabapentin was effective in reducing cough frequency and severity and improving quality of life in patients with RCC but had no effect on capsaicin cough hypersensitivity 82. Gabapentin is usually started at a low dose of 100 mg three times daily and can be increased to a maximum dose of 600 mg three times daily. The other gabapentinoid, pregabalin, in combination with speech pathology also improved cough and quality of life compared to speech pathology therapy alone 83.
Amitriptyline compared to a combination of codeine and guaifenesin for chronic cough after an upper respiratory tract infection caused greater subjective improvements in cough 84. In another trial comparing gabapentin to tricyclic antidepressants (including amitriptyline) in patients with UCC, both neuromodulator classes demonstrated short-term benefit, but most patients in both treatment arms discontinued within 6 months due to tachyphylaxis in treatment effects 85. Side effects are common for patients using neuromodulator therapies and include dizziness, confusion, nausea, dry mouth, and somnolence, often limiting long-term treatment compliance.
P2X3 blocker as a peripheral antitussive.
The purinergic receptors P2X3 and P2X2/3 are expressed by vagal sensory cough fibers and activated by ATP released from airway epithelial cells or inflammatory cells in response to airway injury, infection, or inflammation 86. The first-in-class drug gefapixant displays activity at both P2X3 homomeric and P2X2/3 heteromeric receptors, and a meta-analysis of the clinical trials reported that gefapixant reduced cough frequency by 17.6%, lowered cough severity on a 100 mm visual analog scale by 6.2 mm, and improved Leicester Cough Questionnaire (LCQ) scores by 1.0 point 87. Taste-related events were reported by 69% of participants, with 12% discontinuing because of these side effects, which were due to P2X2/3 receptors that are also expressed by gustatory nerves involved in taste perception 88. There were strikingly large placebo responses, reducing the efficacy of gefapixant. Licensing has been approved in Japan, the United Kingdom, and the European Union but not in the United States.
Camlipixant, a more selective P2X3 antagonist, demonstrated placebo-adjusted reductions in 24 h cough frequency of 34.4% and 34.3% in 50 mg and 200 mg twice daily doses, respectively, after 4 weeks and was accompanied by significant improvement in visual analog scale and LCQ scores, particularly at the 200 mg dose 89. There was less impact on taste due to the selectivity at P2X3 homomeric receptors.
Speech and language therapy.
Behavioral cough suppression treatments have been developed by specialist speech therapists and respiratory physiotherapists. Such treatments involve a multifaceted approach, including educating patients about cough, identifying and managing cough triggers, improving laryngeal hygiene (e.g., avoiding cigarette smoke, excessive alcohol, dehydration, and vocal strain), and training with behavioral cough suppression techniques 90. Randomized controlled studies show improvement in cough counts and quality of life measures 91. Speech and language therapy is now commonly used in parallel with medication in the management of chronic cough.
Potential new emerging antitussives for cough hypersensitivity.
Although preclinical studies have identified transient receptor potential (TRP) channels as targets for cough suppression 3, TRPV1, TRPA1, and TRPV4 antagonists have performed poorly in clinical trials of chronic cough. Agonists at the TRP cation channel subfamily M member 8 (TRPM8), a nonselective cation channel that controls Ca2+ homeostasis and that is responsive to cooling and menthol, are in early-phase trials and may prove useful for providing both short- and long-term relief of chronic cough due to the rapid-onset cooling sensation in the throat. Specific voltage-gated sodium channels that propagate action potentials along vagal sensory nerve fibers may lead to the development of a novel classes of antitussives 92. Selective inhibitors of specific sodium channel subunits, for example, NaV1.7, have shown antitussive activity in guinea pigs 93, and a dry powder formulation of the charged sodium channel blocker NTX-1175 is in early-phase development. Centrally acting compounds such as the alpha-7 nicotinic acetylcholine receptor partial agonist (i.e., bradanicline), neurokinin 1 receptor antagonist (i.e., orvepitant), and the N-methyl-D-aspartic acid receptor allosteric modulator (i.e., ifenprodil) have been studied with no or marginal effects in RCC 94, 95. In a randomized double-blind placebo-controlled crossover trial in patients with IPF, the mixed κ-opioid receptor agonist/μ-opioid receptor antagonist nalbuphine reduced cough severity more than placebo 96.
COUGH HYPERSENSITIVITY NEUROPATHIC DISORDER AS A DISEASE
Significant progress has been made in our understanding of the mechanistic and clinical features of cough hypersensitivity and chronic cough ( Figure 1 ). By acknowledging that cough hypersensitivity represents a key feature of chronic cough, research and clinical efforts became focused on understanding and treating the causative under- lying neural hypersensitivity, advancing the field significantly. However, it has become clear that the causes of neural hypersensitivity are not simply explained by the existence of a known pathology impacting the airways. Thus, although some patients do have chronic cough as a symptom of an underlying disease impacting their airways, this view of cough is arguably too restricted and no longer adequate to manage all patients, especially those with RCC or UCC. The evidence for neuropathological causes of chronic cough in such patients suggests that an alternative perspective is needed, and this is further supported by the often-unsatisfactory clinical outcomes resulting from focusing cough management therapies on presumed peripheral disease causes 97. The cough hypersensitivity neuropathic disorder underlying chronic cough should be considered as a distinct disease that requires different and dedicated approaches to clinical management.
A reassessment of RCC and UCC in specific respiratory conditions in terms of the heterogeneity of the hypersensitive pathways 98, and in terms of understanding the mechanisms of hypersensitivity and new effective antitussive therapies 99, is needed. Acknowledging that cough can be a neuropathic or nociplastic disease also reduces the risk of underestimating the physical, psychological, and social impact that chronic cough directly poses on patients. It encourages healthcare providers to consider these features of chronic cough more seriously as part of a spectrum of neurological complications. Chronic pain, another example of a sensory hypersensitivity, has been redefined as a disease with primary and secondary causes, resulting in improvements in clinical management, epidemiological investigations, policy, and research 100. The imperative to consider chronic cough as a disease seems undeniable 101.
DISCLOSURE STATEMENT
K.F.C. has received research grants from GSK, Merck, and UK Research and Innovation, paid to his institution; personal honoraria for speaking engagements for AstraZeneca, GSK, and Novartis; and personal honoraria for participation on advisory board meetings of AstraZeneca, GSK, Merck, Nocion, Novartis, Reckitt Benckiser, Roche, Shionogi, and Trevi. He is also on the Scientific Advisory Board of The Clean Breathing Institute funded by Haleon. S.B.M. has received honoraria from Bellus Health, Chiesi, Merck, NeRRe Therapeutics, and Reckitt Benckiser, as well as grant support from Bellus Health, Merck, and Reckitt Benckiser, outside of the submitted work.
LITERATURE CITED
1. Song W-J , Chang Y-S , Faruqi S , et al. 2015 . The global epidemiology of chronic cough in adults: a systematic review and meta-analysis . Eur. Respir. J. 45 : 1479 – 8110.1183/ 09031936. 00218714
2. Irwin RS , Carrao WM , Pratter MR. 1981 . Chronic persistent cough in the adult: the spectrum and frequency of causes and successful outcome of specific therapy. Am. Rev. Respir. Dis. 123 : 413 – 17
3. Mazzone SB , Undem BJ. 2016 . Vagal afferent innervation of the airways in health and disease . Physiol. Rev. 96 : 975 – 102410.1152/physrev. 00039. 2015
4. Irwin RS , Curley FJ , French CL. 1990. Chronic cough: the spectrum and frequency of causes, key components of the diagnostic evaluation, and outcome of specific therapy. Am. Rev. Respir. Dis. 141 : 640 – 47 10.1164/ajrccm/141.3.640
5. Chung KF , Pavord ID. 2008 . Chronic cough: prevalence, pathogenesis, and causes. Lancet 371 : 1364 – 74 10.1016/S0140-6736(08)60595-4
6. Chung KF , McGarvey L , Song W-J , et al. 2022. Cough hypersensitivity and chronic cough. Nat. Rev. Dis. Primers 8 : 45 10.1038/s41572-022- 00370-w
7. Irwin RS, Dudiki N, French CL.2020. Life-threatening and non-life-threatening complications associated with coughing: a scoping review. Chest 158 :2058 – 73 10.1016/j. chest.2020. 06.012
8. Dávila I , Puente L , Quirce S , et al. 2023. Characteristics and management of patients with refractory or unexplained chronic cough in outpatient hospital clinics in Spain: a retrospective multicenter study. Lung 201:275 – 86 10.1007/s00 408-023-00620-y
9. Morice AH.2010. The cough hypersensitivity syndrome: a novel paradigm for understanding cough . Lung 188 ( Suppl. 1 ): 87 – 90 10. 1007 /s00408-009-9185-z
10. Chung KF. 2011. Chronic ‘cough hypersensitivity syndrome’: a more precise label for chronic cough. Pulm. Pharmacol. Ther. 24: 267 – 71 10.1016/j.pupt.2011.01.012
11. Chung KF, McGarvey L, Mazzone SB. 2013. Chronic cough as a neuropathic disorder. Lancet Respir. Med. 1 : 414–22 0.1016/S2213-2600(13) 70043-2
12. Widdicombe J, Tatar M, Fontana G, et al. 2011. Workshop: tuning the ‘cough center.’ Pulm. Pharmacol. Ther. 24: 344–52 10.1016/j.pupt. 2010. 12.010
13. Ruhl CR, Pasko BL, Khan HS , et al. 2020. Mycobacterium tuberculosis sulfolipid-1 activates nociceptive neurons and induces cough. Cell 181:293– 305.e11 10.1016/j.cell. 2020.02.026
14. Naqvi KF , Mazzone SB , Shiloh MU. 2023 . Infectious and inflammatory pathways to cough. Annu. Rev. Physiol. 85:71–91 10.1146/annurev-physiol-031422-092315
15. Trevizan-Bau P , Mazzone SB. 2023 . Neuroimmune pathways regulating airway inflammation. Ann.Allergy Asthma Immunol. 131 : 550 – 60 10.1016/j.anai.2023.07.020
16. Shapiro CO , Proskocil BJ , Oppegard LJ , et al. 2021. Airway sensory nerve density is increased in chronic cough. Am. J. Respir. Crit. Care Med. 203: 348 – 55 10.1164/rccm.201912-2347OC
17. Song W-J, Hui CKM, Hull JH , et al. 2021. Confronting COVID-19-associated cough and the post-COVID syndrome: role of viral neurotropism, neuro- inflammation, and neuroimmune responses. Lancet Respir. Med. 9 : 533 – 44 10.1016/S2213-2600(21) 00125-9
18. Ryan NM, Vertigan AE, Ferguson J , et al. 2012. Clinical and physiological features of postinfectious chronic cough associated with H1N1 infection. Respir. Med. 106 : 138 – 44 10.1016/j.rmed.2011.10.007
19. Ando A , Smallwood D , McMahon M , et al. 2016. Neural correlates of cough hypersensitivity in humans: evidence for central sensitisation and dysfunctional inhibitory control. Thorax 71: 23 – 29 10.1136/thoraxjnl -2015-207425
20. Fitzcharles MA, Cohen SP, Clauw DJ, et al. 2021. Nociplastic pain: towards an understanding of prevalent pain conditions . Lancet 397 : 2098 – 110 10.1016/S0140-6736(21)00392-5
21. Namgung E , Song W-J , Kim Y-H , et al. 2022. Structural and functional correlates of higher cortical brain regions in chronic refractory cough .Chest 162:851 – 60 10.1016/j. chest. 2022.04.141
22. Moe AAK , Singh N , Dimmock M , et al. 2024. Brainstem processing of cough sensory inputs in chronic cough hypersensitivity. eBioMedicine 100:104976 10.1016/j.ebiom. 2024. 104976
23. Cho PSP , Fletcher HV , Turner RD , et al. 2019. Impaired cough suppression in chronic refractory cough. Eur. Respir. J. 53 : 1802203 10.1183/ 13993003.02203-2018
24. Mazzone SB , Cole LJ , Ando A , et al. 2011. Investigation of the neural control of cough and cough suppression in humans using functional brain imaging. J. Neurosci. 31 : 2948 – 58 10.1523/ JNEUROSCI.4597-10.2011
25. Manconi M, Garcia-Borreguero D, Schormair B, et al. 2021. Restless legs syndrome. Nat. Rev. Dis. Primers 7: 80 10.1038/s41572-021-00311-z
26. Driessen AK, Devlin A-C, Lundy FT, et al. 2020. Perspectives on neuro- inflammation contributing to chronic cough. Eur. Respir. J. 56 : 2000758 10.1183/13993003.00758-2020
27. Cho PSP , Fletcher HV , Patel IS , et al. 2021. Cough hypersensitivity and suppression in COPD. Eur. Respir. J. 57: 2003569 10.1183/13993003. 03569-2020
28. Mazzone SB, Chung KF, McGarvey L. 2018 . The heterogeneity of chronic cough: a case for endotypes of cough hypersensitivity. Lancet Respir. Med. 6:636 – 46 10.1016/ S2213-2600 (18)30150-4
29. Won H-K , Kang S-Y , Kang Y , et al. 2019. Cough-related laryngeal sensations and triggers in adults with chronic cough: symptom profile and impact. Allergy Asthma Immunol. Res. 11:622–31 10. 4168/aair.2019.11.5.622
30. Hilton E , Marsden P , Thurston A , et al. 2015 . Clinical features of the urge-to-cough in patients with chronic cough. Respir. Med. 109 : 701–7 10.1016/j.rmed.2015 .03.011
31. Morice AH , Jakes AD , Faruqi S , et al. 2014. A worldwide survey of chronic cough: a manifestation of enhanced somatosensory response. Eur. Respir. J. 44 : 1149 – 55 10. 1183/09031936. 00217813
32. Dicpinigaitis PV, Birring SS, Blaiss M, et al. 2023. Demographic, clinical, and patient-reported outcome data from 2 global, phase 3 trials of chronic cough. Ann. Allergy Asthma Immunol. 130:60–66 10.1016/ j.anai.2022. 05.003
33. Çolak Y , Afzal S , Lange P , et al. 2019 . Role and impact of chronic cough in individuals with asthma from the general population. J. Allergy Clin. Immunol. Pract. 7:1783–92.e8 10.1016/j.jaip.2019.02.021
34. Deng SJ , Wang J , Liu L , et al. 2022. Chronic cough in asthma is associated with increased airway inflammation, more comorbidities, and worse clinical outcomes. Allergy Asthma Proc.43:209 – 19 10.2500/aap.2022. 43.220022
35. Kanemitsu Y, Fukumitsu K, Kurokawa R , et al. 2020 . Increased capsaicin sensitivity in patients with severe asthma is associated with worse clinical outcome. Am. J. Respir. Crit. Care Med. 201 : 1068 – 77 10. 1164/ rccm.201911-2263OC
36. Ito K , Kanemitsu Y , Kamiya T , et al. 2023. Functional gastrointestinal disorders are associated with capsaicin cough sensitivity in severe asthma . Allergol. Int. 72: 271 – 78 10.1016/ j.alit.2022. 08.009
37. Hilton ECY , Baverel PG , Woodcock A, et al. 2013. Pharmacodynamic modeling of cough responses to capsaicin inhalation calls into question the utility of the C5 end point. J. Allergy Clin. Immunol. 132: 847 – 55.e5 10.1016/j.jaci.2013. 04.042
38. Vertigan AE , Kapela SL , Gibson PG. 2021. Laryngeal dysfunction in severe asthma: a cross-sectional observational study. J. Allergy Clin. Immunol. Pract. 9: 897 – 905 10.1016/j.jaip.2020. 09.034
39. Drake MG , Scott GD , Blum ED , et al. 2018. Eosinophils increase airway sensory nerve density in mice and in human asthma. Sci. Transl. Med. 10 : eaar8477 10.1126/scitranslmed .ar8477
40. Lin A-H , Athukorala A , Gleich GJ , Lee L-Y. 2019. Cough responses to inhaled irritants are enhanced by eosinophil major basic protein in awake mice. Am. J. Physiol. Regul. Integr.Comp.Physiol. 317 : R93 – 97 10.1152/ajpregu. 00081.2019
41. Mazzone SB , Mori N , Canning BJ. 2005. Synergistic interactions between airway afferent nerve subtypes regulating the cough reflex in guinea pigs. J. Physiol. 569 : 559–73 10.1113/jphysiol.2005. 093153
42. Pratter MR. 2006. Chronic upper airway cough syndrome secondary to rhinosinus diseases (previously referred to as postnasal drip syndrome): ACCP evidence-based clinical practice guidelines. Chest 129 : 63S – 71 S 10.1378/chest. 129.1_ suppl.63S
43. Saleh H. 2009. Rhinosinusitis, laryngopharyngeal reflux and cough: an ENT viewpoint. Pulm. Pharmacol. Ther. 22 : 127 – 29 10. 1016/j.pupt. 2009.01.002
44. O’Hara J , Jones NS. 2006. “ Post-nasal drip syndrome”: most patients with purulent nasal secretions do not complain of chronic cough. Rhinology 44 : 270 – 73
45. Niimi A. 2011. Structural changes in the airways: cause or effect of chronic cough? Pulm. Pharmacol. Ther. 24 : 328 – 33 10.1016/j.pupt. 2011. 01.011
46. Pecova R , Zucha J , Pec M , et al. 2008 Cough reflex sensitivity testing in in seasonal allergic rhinitis patients and healthy volunteers. J. Physiol. Pharmacol. 59 ( Suppl. 6 ): 557 – 64
47. Plevkova J , Brozmanova M , Pecova R , Tatar M. 2006. The effects of nasal histamine challenge on cough reflex in healthy volunteers. Pulm. Pharmacol. Ther.19: 120 – 27 10.1016/j.pupt.2005. 04.004
48. Irwin RS. 2006 . Chronic cough due to gastroesophageal reflux disease: ACCP evidence-based clinical practice guidelines. Chest 129 : 80S –94 S 10.1378/chest.129.1_ suppl. 80S
49. Smith JA , Decalmer S , Kelsall A , et al.2010. Acoustic cough–reflux associations in chronic cough: potential triggers and mechanisms. Gastroenterology 139 : 754 – 62 10.1053/j.gastro.2010.06. 050
50. Qiu Z , Yu L , Xu S , et al. 2011. Cough reflex sensitivity and airway inflammation in patients with chronic cough due to non-acid gastro-oesophageal reflux. Respirology 16 : 645–52 10.1111/j.1440-1843. 2011 . 01952.x
51. Ing AJ , Ngu MC , Breslin AB. 1994 . Pathogenesis of chronic persistent cough associated with gastro- esophageal reflux. Am. J. Respir. Crit. Care Med. 149:160–67 10. 1164/ajrccm.149. 1.8111576
52. Javorkova N , Varechova S , Pecova R, et al. 2008. Acidification of the oesophagus acutely increases the cough sensitivity in patients with gastro-oesophageal reflux and chronic cough. Neurogastroenterol. Motil. 20:119 – 24 10.1111/j. 1365-2982. 2007.01020.x
53. Diener U , Patti MG , Molena D , et al. 2001. Esophageal dysmotility and gastroesophageal reflux disease . J. Gastrointest. Surg. 5 : 260 – 65 10. 1016/S1091-255X(01)80046-9
54. Rubinstein E, Rosen RL. 2018 . Respiratory symptoms associated with eosinophilic esophagitis. Pediatr. Pulmonol. 53 : 1587 – 91 10.1002/ ppul.24168
55. Saunders P , Wu Z , Fahy WA , et al. 2023. The burden and impact of cough in patients with idiopathic pulmonary fibrosis: an analysis of the prospective observational PROFILE study. Ann. Am. Thorac. Soc. 20:1267–73 10.1513/ AnnalsATS.202 302-174OC
56. Lan NSH, Moore I, Lake F. 2021 . Understanding cough in interstitial lung disease: a cross-sectional study on the adequacy of treatment. Intern. Med. J. 51 : 923–29 10. 1111/imj. 14837
57. Green R , Baldwin M , Pooley N , et al. 2024 . The burden of cough in idiopathic pulmonary fibrosis and other interstitial lung diseases: a systematic evidence synthesis . Respir. Res. 25:325 10.1186/ s12931 -024-02897-w
58. Doherty MJ , Mister R , Pearson MG, Calverley PMA. 2000. Capsaicin induced cough in cryptogenic fibrosing alveolitis. Thorax 55 : 1028 – 32 10. 1136/thorax.55.12.1028
59. Jones RM, Hilldrup S, Hope-Gill BDM, et al. 2011. Mechanical induction of cough in idiopathic pulmonary fibrosis. Cough 7 : 2 10. 1186/1745-9974-7-2
60. Chung KF , Birring SS , Morice AH , et al. 2022 . Tackling the neuropathic cough of idiopathic pulmonary fibrosis (IPF): more needs to be done. Lung 200: 673–75 10. 1007/s00408-022-00589-0
61. Madison JM , Irwin RS. 2005. Chronic cough in adults with interstitial lung disease. Curr. Opin. Pulm. Med. 11 : 412–16 10.1097/01. mcp.0000174 249.07762.37
62. Dicpinigaitis PV. 2014 . Effect of viral upper respiratory tract infection on cough reflex sensitivity. J. Thorac. Dis. 6 : S708 – 11
63. Eccles R , Lee PCL. 2004. Cough induced by airway vibration as a model of airway hyperreactivity in patients with acute upper respiratory tract infection. Pulm. Pharmacol. Ther. 17 : 337–42 10.1016/j.pupt.2004.09. 011
64. Kang YR , Huh J-Y , Oh J-Y , et al. 2023. Clinical characteristics of post-COVID-19 persistent cough in the Omicron era. Allergy Asthma Immunol. Res. 15:395–405 10.4168/aair. 2023.15.3.395
65. Xu T , Chen Y , Zhan W , et al. 2024 . Profiles of cough and associated risk factors in nonhospitalized individuals with SARS-CoV-2 omicron variant infection: cross-sectional online survey in China. JMIR Public Health Surveill. 10: e47453 10.2196/47453
66. Martins RHG, de Azevedo ES, Müller JVC, Loli A. 2025. Dysphonia and COVID-19: a review. J. Voice In press. https://doi.org/10.1016/j.jvoice. 2024.11.034
67. Guilleminault L , Mazzone SB , Chazelas P, et al. 2024. Cerebellar ataxia, neuropathy and vestibular areflexia syndrome: a neurogenic cough prototype. ERJ Open Res.10 : 00024 – 2024
68. Beecroft SJ , Cortese A , Sullivan R , et al. 2020. A Māori specific RFC1 pathogenic repeat configuration in CANVAS, likely due to a founder allele. Brain 143: 2673–80 10.1093/brain/ awaa203
69. Huin V, Coarelli G, Guemy C , et al. 2022. Motor neuron pathology in CANVAS due to RFC1 expansions. Brain 145: 2121 – 32 10.1093/brain/awab449
70. Dicpinigaitis PV, Kantar A, Enilari O, Paravati F. 2018. Prevalence of Arnold nerve reflex in adults and children with chronic cough. Chest 153:675 –79 10.1016/j.chest.2017. 11.019
71. Guilleminault L , Chazelas P , Melloni B , et al. 2023. Repeat expansions of RFC1 in refractory chronic cough: a missing piece of the puzzle? Chest 163:911– 15 10.1016/j.chest. 2022. 11.014
72. Hirons B , Cho PSP , Rhatigan K , et al. 2025. Repeat expansions in RFC1 gene in refractory chronic cough. ERJ Open Res. 11 : 00584 – 2024 10.1183/23120541.00584-2024
73. North RY , Odem MA , Li Y , et al. 2022. Electrophysiological alterations driving pain-associated spontaneous activity in human sensory neuron somata parallel alterations described in spontaneously active rodent nociceptors. J. Pain 23 : 1343 – 57 10.1016/j.jpain.2022.02.009
74. Tan AM, Samad OA, Dib-Hajj SD, Waxman SG. 2015. Virus-mediated knockdown of Nav1.3 in dorsal root ganglia of STZ-induced diabetic rats alleviates tactile allodynia. Mol. Med. 21:544–52 10.2119/molmed. 2015. 00063
75. Dalal A , Tata M , Allègre G , et al. 1999. Spontaneous activity of rat dorsal horn cells in spinal segments of sciatic projection following transection of sciatic nerve or of corresponding dorsal roots. Neuroscience 94 : 217 –28 10.1016/S0306-4522(99) 00328-0
76. Morice AH, Millqvist E, Bieksiene K, et al. 2020 . ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. Eur. Respir. J. 55 : 1901136 10.1183/ 13993003.01136-2019
77. Irwin RS, Baumann MH, Bolser DC, et al. 2006. Diagnosis and management of cough executive summary: ACCP evidence-based clinical practice guidelines. Chest 129 : 1S – 23 S 10. 1378/chest.129.1_suppl.1S
78. Morice AH, Menon MS, Mulrennan SA, et al. 2007. Opiate therapy in chronic cough. Am. J. Respir. Crit. Care Med. 175 : 312 – 15 10.1164/ rccm.200607-892OC
79. Oh J-Y , Kang S-Y , Kang N , et al. 2024. Characterization of codeine treatment responders among patients with refractory or unexplained chronic cough: a prospective real-world cohort study. Lung 202 : 97 – 106 10.1007/ s00408-024-00674-6
80. Ryan NM , Vertigan AE , Birring SS. 2018. An update and systematic review on drug therapies for the treatment of refractory chronic cough. Expert Opin. Pharmacother. 19 : 687 – 711 10.1080/14656566. 2018.1462795
81. Papassidero P , Wichert-Ana L , Lia EN , et al. 2023. Pharmacodynamic effect of gabapentin on central nervous system in patients with chronic low back pain: a [99mTc]Tc-ECD SPECT study. Reg. Anesth Pain Med. 48 : 408 – 13 10.1136/rapm-2022-104047
82. Ryan NM , Birring SS , Gibson PG. 2012. Gabapentin for refractory chronic cough: a randomised, double-blind, placebo-controlled trial. Lancet 380:1583–89 10. 1016/S0140-6736(12)60776-4
83. Vertigan AE , Kapela SL , Ryan NM , et al. 2016 . Pregabalin and speech pathology combination therapy for refractory chronic cough: a randomized controlled trial . Chest 149 : 639 – 48 10.1378/chest.15-1271
84. Jeyakumar A , Brickman TM , Haben M. 2006. Effectiveness of amitriptyline versus cough suppressants in the treatment of chronic cough resulting from postviral vagal neuropathy . Laryngoscope 116 : 2108 – 12 10. 1097/01.mlg.0000244377.60334.e3
85. Bowen AJ , Nowacki AS , Contrera K , et al. 2018. Short- and long-term effects of neuromodulators for unexplained chronic cough. Otolaryngol. Head Neck Surg. 159 : 508–15 10.1177/ 01945998187 68517
86. Kollarik M , Ru F , Undem BJ. 2019 . Phenotypic distinctions between the nodose and jugular TRPV1-positive vagal sensory neurons in the cynomolgus monkey . NeuroReport 30 : 533 – 37 10.1097/WNR.0000 000000001231
87. Kum E , Patel M , Diab N , et al. 2023. Efficacy and tolerability of gefapixant for treatment of refractory or unexplained chronic cough: a systematic review and dose-response meta-analysis . JAMA 330 : 1359–69 10.1001/jama.2023. 18035
88. Smith JA , Kitt MM , Morice AH , et al. 2020 . Gefapixant, a P2X3 receptor antagonist, for the treatment of refractory or unexplained chronic cough: a randomised, double-blind, controlled, parallel-group, phase 2b trial . Lancet Respir. Med. 8 : 775 – 85 10.1016/S2213-2600(19) 30471-0
89. Smith JA , Birring SS , Blaiss MS , et al. 2025 . Camlipixant in refractory chronic cough: a phase 2b, randomized, placebo-controlled trial (SOOTHE) . Am. J. Respir. Crit. Care Med. 211 : 1038 – 48 10.1164 /rccm.202409-1752OC
90. Vertigan AE, Haines J, Slovarp L. 2019. An update on speech pathology management of chronic refractory cough. J. Allergy Clin. Immunol. Pract. 7 : 1756 – 61 10. 1016/j.jaip.2019.03.030
91. Yi B , Wang S , Xu X , Yu L. 2024 . Efficacy of behavioral cough suppression therapy for refractory chronic cough or unexplained chronic cough: a meta-analysis of randomized controlled trials . Ther. Adv. Respir. Dis. 18 : 17534666241305952 10.1177/175 34666241305952
92. Sun H , Kollarik M , Undem BJ. 2017 . Blocking voltage-gated sodium channels as a strategy to suppress pathological cough. Pulm. Pharmacol. Ther.47:38–41 10.1016/j.pupt. 2017.05.010
93. Tochitsky I , Jo S , Andrews N , et al. 2021 . Inhibition of inflammatory pain and cough by a novel charged sodium channel blocker . Br. J. Pharmacol. 178:3905–23 10. 1111/bph.15531
94. Kanemitsu Y , Smith J , Butera P , et al. 2020. The efficacy of bradanicline in refractory chronic cough. Eur. Respir. J. 56 : 4654
95. Smith J , Allman D , Badri H , et al. 2020. The neurokinin-1 receptor antagonist orvepitant is a novel antitussive therapy for chronic refractory cough: results from a phase 2 pilot study (VOLCANO-1) . Chest 157:111 – 18 10.1016/j. chest.2019.08.001
96. Maher TM , Avram C , Bortey E , et al. 2023. Nalbuphine tablets for cough in patients with idiopathic pulmonary fibrosis. NEJM Evid.2 :EVIDoa2 300083 10.1056/EVIDoa 2300083
97. Brindle K , Morice A , Carter N , et al. 2023. The “vicious circle” of chronic cough: the patient experience –qualitative synthesis . ERJ Open. Res. 9 : 00094 – 2023
98. Song W-J , Chung KF. 2020 . Exploring the clinical relevance of cough hypersensitivity syndrome . Expert Rev. Respir. Med. 14 : 275 – 84 10.1080/17476348.2020.1713102
99. Mazzone SB , Satia I , McGarvey L , et al. 2022 . Chronic cough and cough hypersensitivity: from mechanistic insights to novel antitussives. Lancet Respir. Med. 10 : 1113 – 15 10.1016/S2213-2600(22)00404-0
100. Treede R-D , Rief W , Barke A , et al. 2019 . Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11) . Pain 160 : 19 – 27 10.1097/j.pain. 0000000000001384
101. Chung KF , Mazzone SB , McGarvey L , Song W-J. 2025 . Chronic cough as a disease: implications for practice, research, and health care . Lancet Respir. Med. 13 : 110 – 12 10.1016/S2213-2600(24)00422-3
Credits: Kian Fan Chung, Stuart B. Mazzone. 2026. Chronic Cough Hypersensitivity as a Neuropathic Disorder: Implications for Management and New Treatments. Annual Review Medicine. 77:449-462. https://doi.org/10.1146/annurev-med-050224-124414






