

Ige OT, Ige SO1, Olayinka AT2
Department of Medical Microbiology, College of Medicine, Kaduna State University, 1Department of Paediatrics, Yusuf Dantsoho Hospital, Kaduna, 2Department of Medical Microbiology, Ahmadu Bello University, Zaria, Kaduna State, Nigeria
Address for correspondence: Dr. Ige OT,
Department of Medical Microbiology, College of Medicine, Kaduna State University, Kaduna, Kaduna State, Nigeria.
E-mail: anjolaoluwanow@gmail.com
ABSTRACT
Background: Chlamydia trachomatis infections are the most prevalent bacterial sexually transmitted infections recognized globally. There is a paucity of data on the prevalence of C. trachomatis infection in Northern Nigeria. This research was conducted with the objective of determining the prevalence of genital C. trachomatis infection among females in the reproductive age group.
Materials and Methods: Three hundred and sixty-five patients were enrolled in this study. Patients were administered questionnaires requesting information on biomedical, sociodemographic data. Endocervical specimens were collected, subjected to DNA extraction and polymerase chain reaction (PCR) using primers from Inqaba Biotechnical industries, South Africa. Data management was done using SPSS software version 20.0 statistical package.
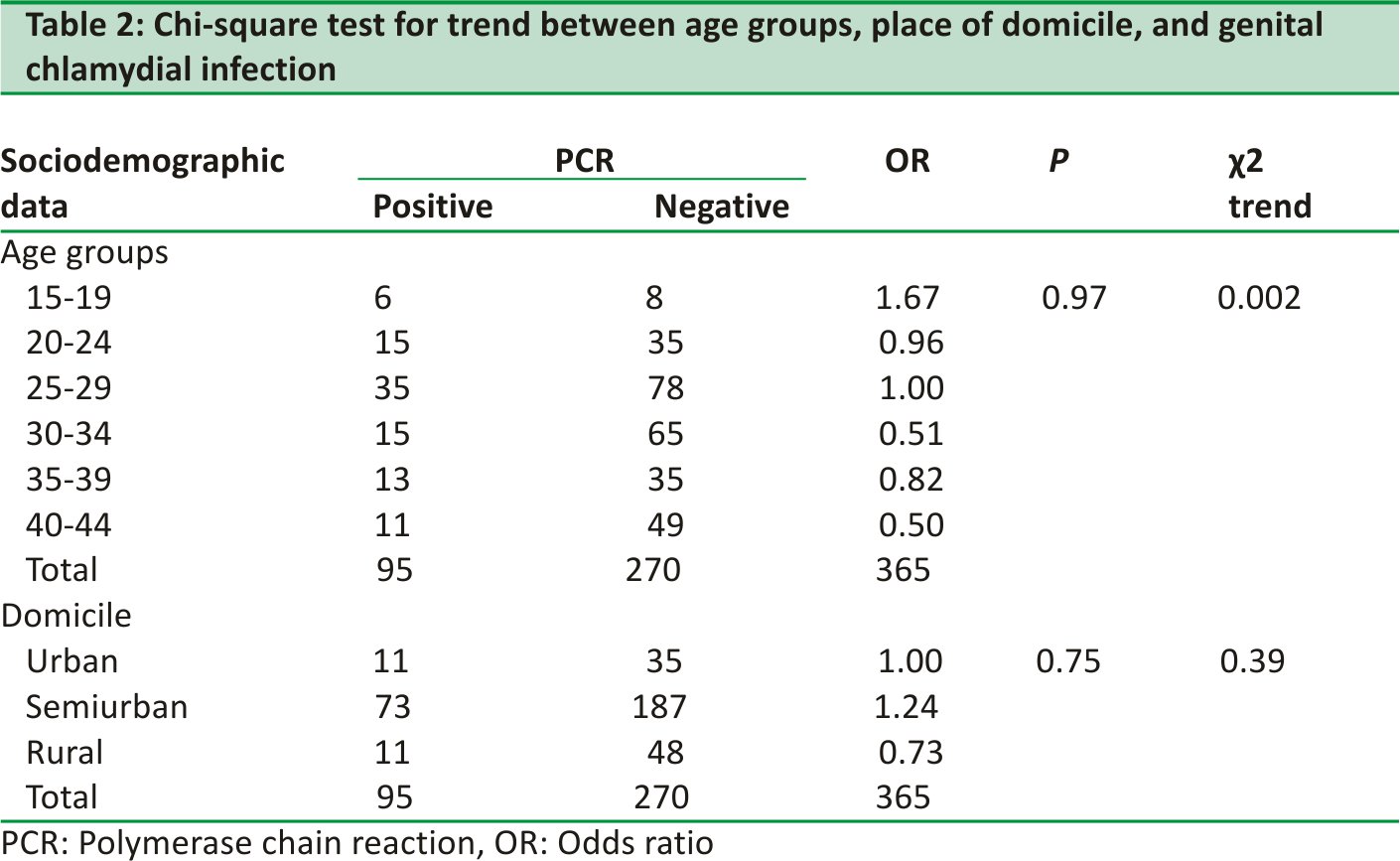
Results: Of the 365 patients studied, 95 of them had positive results by the PCR assay, giving 26% prevalence for genital C. trachomatis infection among women of reproductive age group. Associated risk factors for genital chlamydia infection identified include low educational status, early age at sexual debut, early age at marriage, and lack of use of condoms during sexual intercourse. The frequency of positive results was found to be higher among the age group 25‑29 years, those living in suburban areas and the unmarried [Tables 1 and 2].
Conclusion: A prevalence of 26% was found, in this study, for genital C. trachomatis infection among women of reproductive age group. Risk factors include as follows: low educational status, early age at sexual debut, early age at marriage, and lack of use of protection during sexual intercourse.
Keywords: Chlamydia trachomatis, Nigeria, prevalence, reproductive age‑ group, women, Zaria
INTRODUCTION
Infections caused by Chlamydia trachomatis are now recognized as the most prevalent and are among the most damaging, of all sexually transmitted diseases (STDs). Over 100 million chlamydia infections are detected worldwide annually.
C. trachomatis is a small obligate intracellular bacterium transmitted by sexual intercourse. It is a cause of endocervicitis and also a pelvic inflammatory disease in women.1‑3 Chlamydia infection of the genital tract is seen most frequently in young women who are sexually active.
The majority of C. trachomatis genital tract infections are mild or asymptomatic in up to 80% of women, making detection and diagnosis difficult and this can lead to sequelae such as tubal damage, tubal infertility, and ectopic pregnancy.3,4
In Northern Nigeria, reliable data on the prevalence of genital Chlamydia infection and information regarding the prevalence rate of C. trachomatis is limited.4 This may be partly due to the lack of personnel expertise with regard to isolation in cell culture and polymerase chain reaction (PCR) techniques, and the high cost of facilities required for making a diagnosis of C. trachomatis infection.5,6 Thus, severe complications may likely be more frequently encountered.
Of the various diagnostic techniques available, Nucleic acid amplification tests are the most sensitive and specific. PCR offers an accurate, rapid, and reliable method for the detection of C. trachomatis.5
This study was aimed to determine the prevalence of genital C. trachomatis among women of the reproductive age group attending the General Out‑patient Clinic Ahmadu Bello University Teaching Hospital, Zaria.
MATERIALS AND METHODS
This study was carried out between February and July 2013 at the Ahmadu Bello University Teaching Hospital, Shika‑ Zaria, Kaduna State, Nigeria. Participants were female volunteers aged 18–44 years, attending the General Outpatient Clinic. Women who had taken antibiotics within the preceding 6 weeks and patients who refused to give consent for inclusion into the study were excluded from the study. Ethical approval was obtained from the hospital’s research and ethics committee.
Consenting female patients were consecutively recruited for the study until the sample size of 365 was achieved as calculated using the Fisher formula for sample size determination.6 Patients were required to fill in questionnaires that detailed predisposing/risk factors associated with genital chlamydia infection.
Endocervical swabs were collected from the patients using sterile plastic‑ shaft dacron swabs. Samples were stored in a laboratory freezer at −70°C. The endocervical specimen were pooled, and PCR assay was performed at the Center for Biotechnology Research and Training, Ahmadu Bello University.
Deoxyribonucleic acid from lysate (using the protein kinase extraction method) prepared from the endocervical swabs following thawing was bound to spin columns, washed eluted, and resolved by agarose gel electrophoresis. PCR assay, using primers obtained from Inqaba Biotechnical industries, South Africa, was carried out on the endocervical specimens.
Nested PCR was used to amplify 236‑bp and 205‑bp amplicons targeting the VD2 region of C. trachomatis outer membrane protein A (omp A) gene. Forward outer primer CTS (5’‑3’AATATT GGGATCGTTTG) Reverse outer primer CTA (5′‑3’CCCATCCCAAAGCTGC) Forward inner primer (CTSN 5’‑3’ TTGATGTATTTG TACAT) Reverse inner primer (CTAN5’‑3’ GCTGCCGAGCCCACCT)
The amplified products were observed following electrophoresis in 1.2% agarose gel. The Medicare GELSTAN UV illuminator was used to view DNA and bands corresponding to the gene of interest on the DNA ladder were documented as positive, and those that do not meet this criterion were recorded as negative [Figure 1].
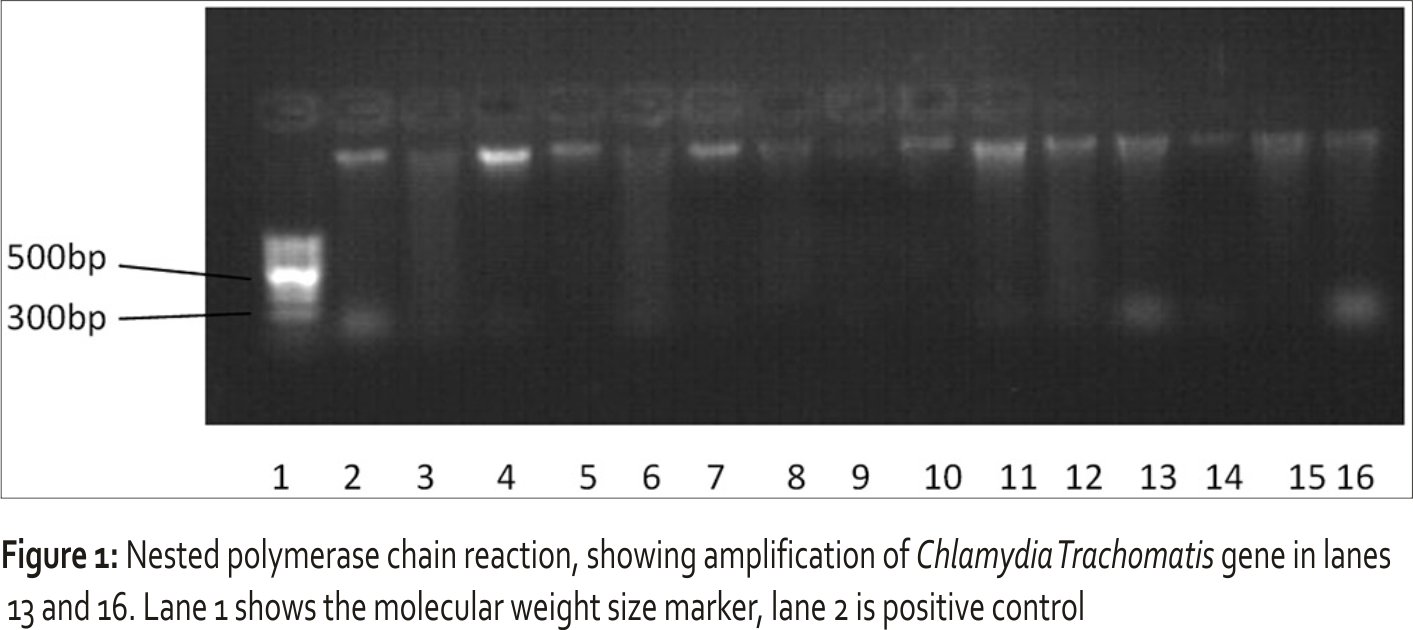
The 205‑bp amplicon of the VD2 region of C trachomatis (Inqaba Biotechnical industries, South‑Africa,) is specific and this was determined using the DNA ladder (Inqaba Biotechnical industries, South Africa,) which was ran alongside the PCR product and served as a basis for further identification of the ompA gene. This served as quality control for the reaction.
Data analysis was performed using SPSS statistical software, version 2.0. Statistical significance was determined at a confidence level of 95%. For bivariate analysis, exposure and outcome variables were cross‑tabulated to compute prevalence odds ratios (ORs) and their corresponding 95% confidence intervals (Cis).
RESULTS
Of the 365 patients studied, 95 of them had positive results for genital C. trachomatis infection by the PCR assay, giving a prevalence value of 26%. Genital chlamydia infection was associated with early age at sexual debut, early age at marriage, more than one sexual partners, and education [Tables 1 and 2].
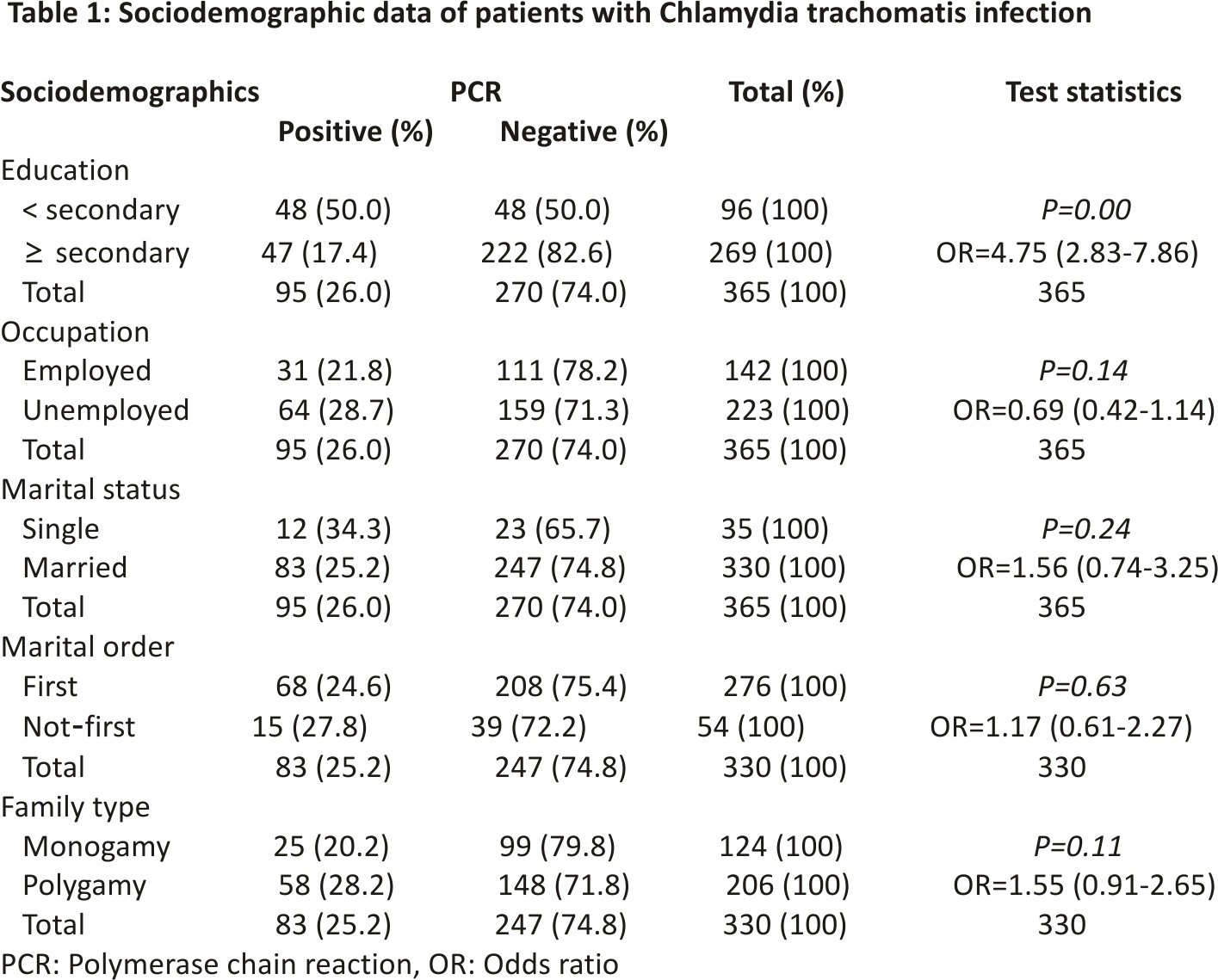
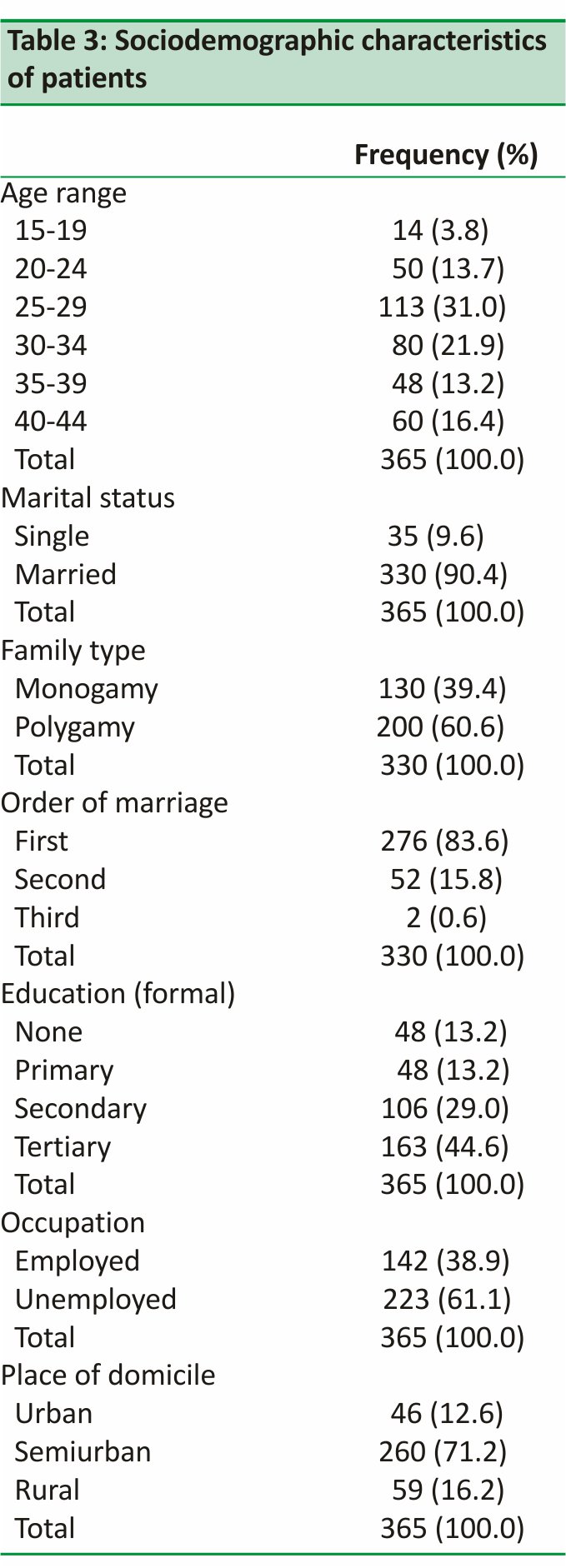
The study did not find statistical significance for most sociodemographic characteristics considered in the patients studied, except for educational status. No statistical significance was found for marital status, family type, marital order, place of domicile, and patients’ employment status [Tables 1 and 3].
Of the 95 PCR positive assay for C. trachomatis, 53 (55.8%) had their first sexual exposure before or at the age of 17 and are about 2.4 times more likely to have C. trachomatis than those who had their first sexual exposure at or after the age of 18 [Table 4].
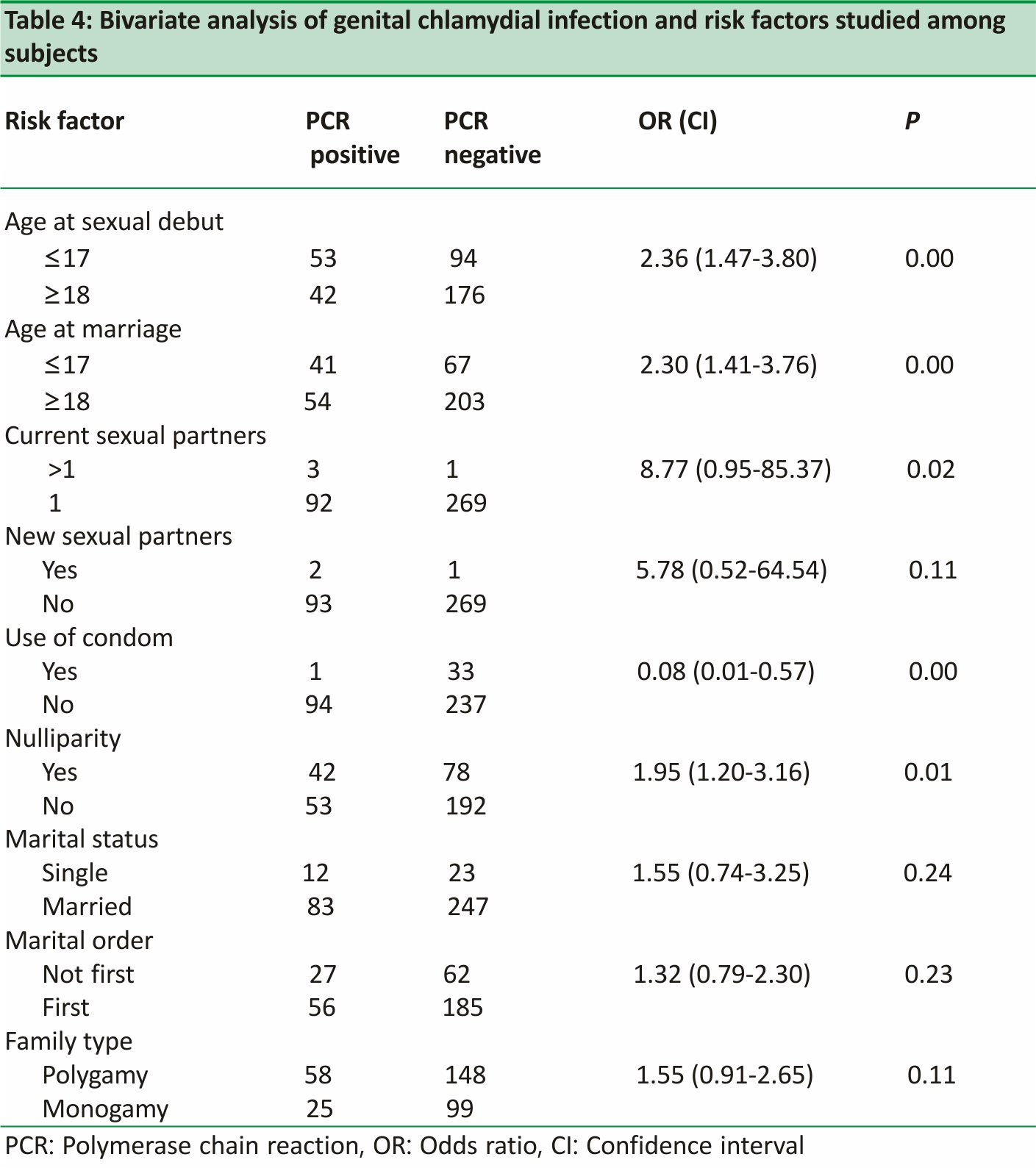
Similarly, 41 (43.2%) of the positive results were from patients who married before or at the age of 17. They were also found to be 2.3 times more prone to having genital chlamydia infection than patients who married at or after 18 years. This was statistically significant [Table 4].
About 44.2% of nulliparous patients had positive results for C. trachomatis genital infection. This finding was statistically significant [Table 4]. Only one out of 34 patients who reported the use of condom during sexual activity, was found to be positive for genital chlamydia infection, this finding was statistically significant [Table 4].
Four patients reported having multiple sexual partners, of which 3 (75%) tested positive for C. trachomatis infection. This was statistically significant [Table 4]. There was no statistical significance found for new sexual partners, that is those who just got new partners after parting with old ones.
DISCUSSION
The prevalence of genital C. trachomatis infection among women of reproductive age group, attending the general out patients’ Department of Ahmadu Bello University Teaching Hospital, was 26%. This finding is lower than that (38.3%). reported by Tukur et al.4 in a previous study done at the same facility on women with tubal infertility, and even much lower than the 51.6% reported by Mawak et al.7 in the study of genital C. trachomatis infection among gynecologic patients in Jos.
At the Lagos University Teaching Hospital, prevalence rates ranged from 18.2% to 51% among women attending the antenatal clinic and those undergoing evaluation for infertility.8,9 These differences could be explained by the fact that those studies were conducted on cohorts of high‑risk groups. The prevalence gotten in this study is in agreement with that reported from the Northeast zone of Nigeria (27%)10 and that of the University college hospital, Ibadan (26.7%).11
Patients within the 25–29 years accounted for the modal age group in this study [Table 2]; hence, it was not surprising that the highest frequency of positive results was found among them, 35 (36.8%). Although the modal age group was similar to the finding reported by Mawak et al.,7 this is contrary to documented reports, that the most common demographic correlate of C. trachomatis infection is among ages <20 years.12
Meanwhile, younger age at sexual debut and at first marriage (≤17) revealed a statistically significant association with C. trachomatis infection. Patients with both factors were 2.4 times more at risk of the infection than those older (P = 0.00, OR 2.36, CI: 1.47–3.80 and P = 0.00 OR 2.30, CI 1.40–3.76, respectively) [Table 4]. A previous study also found that early age at first sexual intercourse was associated with having genital chlamydia infection.13 Early exposure to sex may be a risk factor because the epithelial cells of the immature cervix are, particularly vulnerable to infection by C. trachomatis.14
This study found high educational status to be protective against the infection. Patients with low educational level are about 4.8 times more likely to be infected with genital C. trachomatis infection. This finding is statistically significant (P = 0.00, OR = 4.75, CI: 2.83–7.86) and in agreement with the previous study done by Faber et al.13
The reason for this finding may be due to a higher level of awareness of STDs and knowledge of personal protective measures such as the use of barrier contraceptive to prevent STDs and unwanted pregnancies.15 Among the 34 women who consistently used condoms during sexual intercourse, only one had a positive result for C. trachomatis while 94 (28.4%) of those who do not use condoms regularly were infected [Table 4]. This was statistically significant, (P = 0.00, OR = 0.08, CI ‑ 0.01–0.57) This agrees favourably with similar findings in previous studies.13,16,17 Use of condom, therefore, seems to be a protective factor, while lack of its use is a risk factor as elucidated by this study.
With regard to parity, there was a significant statistical association found for nulliparity, (P = 0.01, OR = 1.95, CI: 20–3.16), this variable was examined in patients who had been married for over 1 year. This was tentatively considered infertility. This finding compares favourably with those of previous studies.4
Multiple sexual partners were also found to have a significant statistical association with genital Chlamydia infection, those with multiple sexual partners were about 8.9 times more likely to be infected with C. trachomatis (P = 0.02). No statistical significance was found for having a new sex partner within the past 3 months. However, these findings should be taken cautiously because the patients who gave information with regard to both variables, (that is multiple sexual partners and new sexual partners) compared to the sample population were too few to rely on the conclusion obtained.
Faber et al.13 in their study reported a statistically significant association between being single and genital chlamydia infection. This is consistent with the findings of this study in which being single, though did not show any statistically significant association, had a higher proportion of positive results (34.3%) No statistical significance was found for family type and marital order.
Generally speaking, the documented prevalence of genital chlamydia infections differs considerably depending on the methodologies, (isolation in cell culture, antigen detection using direct fluorescent antibody assay, and enzyme immunofluorescent assay), used for the identification of C. trachomatis, leading to different prevalence rates even in similar populations. Amplification methods as used in this study have the advantage of a better sensitivity than culture and allows the detection of infection even in individuals with a low number of infectious units, which may be difficult using other methods.
CONCLUSION
Genital C. trachomatis infection was found to be highly prevalent (26.0%) among females of the reproductive age group attending the GOPC, ABUTH, Zaria. Associated risk factors identified with the infection include; low level of education, early age at sexual debut, early age at marriage, multiple sexual partners, and nulliparity. Singles and adolescents are more predisposed to chlamydia genital infections, while the use of condom was a protective factor.
A fundamental requisite for the control and prevention of Chlamydia infection is a national surveillance and screening system. This provides quantitative estimates of incidence and prevalence, a basis for determining secular trends, and a tool for evaluating control efforts.
All sexually active women within the reproductive age group should, therefore, be screened, in an attempt to determine the actual prevalence rate at the local, state and national level, and appropriate control measures constituted to stem the tide of the silent epidemic.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
1. Paavonen J, Eggert‑Kruse W. Chlamydia trachomatis: Impact on human reproduction. Hum Reprod Update 1999; 5:433‑47.
2. World Health Organization, 2011. Prevalence and Incidence of selected sexually transmitted diseases. Available at http: //whqlibdoc.who.int/publications/2011/9789241502450_eng.pdf. [Last accessed on 2017 Oct 30].
3. Land JA, Van Bergen JE, Morré SA, Postma MJ. Epidemiology of Chlamydia trachomatis infection in women and the cost‑effectiveness of screening. Hum Reprod Update 2010; 16:189‑204.
4. Tukur J, Shittu SO, Abdul AM. A case-control study of active genital Chlamydia trachomatis infection among patients with tubal infertility in Northern Nigeria. Trop Doct 2006;36:14‑6.
5. Watson EJ, Templeton A, Russell I, Paavonen J, Mardh PA, Stary A, et al. The accuracy and efficacy of screening tests for Chlamydia trachomatis: A systematic review. J Med Microbiol 2002;51:1021 ‑31.
6. Araoye MO, editor. Sample size determination. In: Research Methodology with Statistics for Health and Social Sciences. Ilorin, Nigeria: Nathadex; 2003. p. 115‑21.
7. Mawak JD, Dashe N, Agabi YA, Panshak BW. Prevalence of genital Chlamydia trachomatis infection among gynaecologic clinic attendees in Jos Nigeria. Shirez E Med J 2011;12:5‑7.
8. Oloyede OA, Fakoya TA, Oloyede AA, Alayo AM. Prevalence and awareness about chlamydial infection in women undergoing infertility evaluation in Lagos Nigeria. Int J Health Res 2009;2:157‑62.
9. Aladesanmi AF, Mumtaz G, Mabey DC. Prevalence of cervical Chlamydial infection in antenatal clinic attenders in Lagos, Nigeria. Genitourin Med 1989;65: 130.
10. Esumeh FI, Agbonlahor D, Okoror L. Chlamydial activity in North-East zone of Nigeria. East J Med 2009;14:10‑6.
11. Darougar S, Forsey T, Osoba AO, Dines RJ, Adelusi B, Coker GO, et al. Chlamydial genital infection in Ibadan, Nigeria. A seroepidemiological survey. Br J Vener Dis 1982;58:366‑9.
12. CDC Sexually Transmitted Diseases Surveillance 2010: Chlamydia. Atlanta, GA: US Department of Health and Human Services, CDC; 2010. Available from: http://www.cdc.gov/std/ stats 07/ toc.htm. [Last accessed on 2011 Jul 10].
13. Faber MT, Nielsen A, Nygård M, Sparén P, Tryggvadottir L, Hansen BT, et al. Genital chlamydia, genital herpes, Trichomonas vaginalis and gonorrhoea prevalence, and risk factors among nearly 70,000 randomly selected women in 4 Nordic countries. Sex Transm Dis 2011;38:727‑ 34.
14. Black CM. Current methods of laboratory diagnosis of Chlamydia trachomatis infections. Clin Microbiol Rev 1997;10: 160‑84.
15. Sexually Transmitted Diseases, Treatment Guidelines 2010. Diseases characterized by Urethritis and Cervicitis. Available at http://www.cdc.gov/std/treatment/2010 urethritis-and-cervicitis.htm. [Last accessed on 2017 Nov 01].
16. Ngandjio A, Clerc M, Fonkoua MC, Thonnon J, Njock F, Pouillot R, et al. Screening of volunteer students in Yaounde (Cameroon, central Africa) for Chlamydia trachomatis infection and genotyping of isolated C. trachomatis strains. J Clin Microbiol 2003; 41:4404‑7.
17. Cates W Jr., Wasserheit JN. Genital chlamydial infections: epidemiology and reproductive sequelae. Am J Obstet Gynecol 1991;164: 1771‑81.
Credits: Ige OT, Ige SO, & Olayinka AT. (2018). Prevalence of Chlamydia Trachomatis infection among women of reproductive age group in a tertiary hospital in Northern Nigeria. Ann Trop Pathol, 9(1), 17-21. DOI:10.4103/atp.atp_ 35_17
: an evolving threat to the Nigerian health system – a review")



: an evolving threat to the Nigerian health system – a review")

